Research Article - (2015) Volume 4, Issue 2
Purpose: To describe and evaluate normal adult dog dentition and temporomandibular joint anatomically and histologically in comparison to humans.
Method: Five adult dogs (6-12 months old) were used in this study. The following anatomical structures were histologically evaluated in a qualitative fashion: Teeth and related bony structures mandible, mandibular condyle, disc, Zygomatic arch, temporal bone, glenoid fossa, retrodiscal tissue and synovia. The macroscopical and microscopic study of the human TMJ was based on the current literature.
Results: Dogs have three Incisors, one canine, four premolars, and 2 molars in the upper and 3 molars in the lower jaw. The TMJ is surrounded by a thin fibrous tissue capsule, and a synovial lining. The mandibular angle has a prominent shape. The glenoid fossa is flat, with extended mediolaterally with retroarticular process. Histologically, the TMJ is composed of different tissues that comprise the mandibular head, mandibular fossa and fibrocartilaginous disc. A layer of fibrous tissue covers the articulating cortical condyle and temporal bone followed by a layer of hyaline cartilage.
Conclusion: Morphologically and numerically dog's teeth are different from humans. Morphologically and histologically, the articular structure of dogs is, on the whole, similar to that of humans. In these animals there is no articular eminence, but they have a retroarticular process.
Animals are being used in research and experiments in an attempt to find a cure for many diseases and disorders that are affecting the humans. Historically animal testing was found in the writings of the Greeks in the second and fourth centuries Before Christ. One of the pioneers to perform experiments on living animals was Aristotle [1]. Where Galen is known as the "father of vivisection because he dissected pigs and goats [2]. Moorish Spain used animals as an experimental method of testing surgical procedures before applying them to human patients [3]. Louis Pasteur demonstrated the germ theory of medicine by inducing anthrax in sheep [4]. In the 1890s, Ivan Pavlov used dogs to describe classical conditioning [5]. Insulin was first isolated from dogs in 1922 [6]. Using armadillos in the 1970s, antibiotic treatments and vaccines for leprosy were developed [7,8].
Dogs as experimental animals
Dogs have been used for ages in surgical research, drug testing and in researching dog's disorders that are similar to human diseases [9]. It has been used as a model for many human conditions as cardiovascular research, diabetes mellitus, ulcerative colitis, open-heart surgery, organ transplantation, pharmacology and toxicology [10]. The dog is one of the most frequently used large animal species for musculoskeletal and dental research. Unlike other animal species, there is a considerable amount of literature comparing canine and human bone to be used as a model for human orthopedic conditions [11]. The highly tractable nature of dogs can be beneficial during the postoperative healing phase where they may be trained to take an active part in recuperative protocols [11].
Dog's teeth
Dogs are "diphyodont" having two sets of teeth, "28 deciduous teeth" being shed and replaced by a "42 permanent ones" set [12]. Dogs have no deciduous precursor for the first premolar a single tooth erupts here at about 5 months [13].
Dog's teeth have thin enamel, probably because carnivores eat nonabrasive food and chew little. The enamel has a lower inorganic content 90% than that of human teeth, a factor that makes the teeth more opaque and whiter in appearance (Table 1 and 2).
| Dental Formulae | |||||
|---|---|---|---|---|---|
| Deciduous | I 3/3 | c1/1 | p3/3 | M2/3 | =14 |
| Permanent | I3/3 | c1/1 | p3/3 | M2/3 | =14 |
Table 1: Dental formulae.
| Tooth Eruption | ||
|---|---|---|
| Deciduous | Permanent | |
| Incisors | 4-6 weeks | 3-5 months |
| Canine | 5-6 weeks | 4-6 months |
| Premolars | 6 weeks | 4-5 months |
| Molars | 5-7 months[14] | |
Table 2: Tooth eruption.
Temporomandibular joint (TMJ)
The temporomandibular joint is a group of anatomic structures that, with a special group of muscles, is responsible for the movement of the mandible during mastication [15]. It is classified as a hinge-sliding joint; it has a unique structure and function. It consists of the condylar process of the mandibular ramus, the mandibular fossa of the temporal bone, a thin articular disc, and a loose joint capsule, which is strengthened by a fibrous lateral ligament. [16] TMJ is a cardinal feature that defines the class Mammalia and separates mammals from other vertebrates [17], its structure is interesting because of its constituent bones, the mandible and the squamous temporal, are intramembranous in origin. Thus, the tissue that covers each articulating surface is a secondary cartilage with a fibrous skin, derived from the periosteum.
Five young mongrel dogs with fully erupted deciduous teeth, aged between 3-4 months and weighing about 5-7 kg were used. Three of the five animals were used to study the anatomical features of dentition and TMJ components, while the other two were used for the histological investigation of the TMJ.
For anatomical dissection, extraction of teeth and histological procedure the animals were euthanized by over doses of anesthesia, ketamine intra muscular injection (normal dose 3-8 milligram/kg body weight). [18] Heads were decapitated, then skin removed and heads were washed.
Gross anatomy of dentition and TMJ
Dentition features
Anatomical features of dentition regarding the number of the different groups of teeth, shape of crown and number, and shape of roots were examined after complete removal of the soft tissues surrounding the jaws.
TMJ bony components and their relations to each other
Soft tissues were removed by scalpel and scissors. The remaining tissue remnants adherent to the bone were removed by boiling the skulls in water then bleaching with 30% H2O2 solution [19].
Soft tissue components of the TMJ (Macroscopical procedure)
Dissection was performed, using a surgical instrument, starting from the external surface, observing all anatomic structures related to the TMJ. The following tissues were removed: Subcutaneous tissue, blood vessels, nerves, parotid gland, masseter muscle, temporalis muscle and adipose tissue. For comparing our results with the human TMJ, we based our description of the human TMJ on specific literature [16,20,21]. Photographs were taken to illustrate details of dentition and TMJ anatomy using Canon PowerShot A3300IS digital camera
Tissue preparation for histological procedures
(Tissue Preparation for light microscopic procedures) [22] -Blocks of tissue containing the TMJs on both sides were isolated and dissected out using a band saw. Following excision, tissues were immediately fixed in 10% neutral buffered formalin for 24 hours, transferred to 70%, 90%, absolute ethanol, then xyline and embedded in paraffin. Sections were cut to 4 μm thickness and processed for standard staining with haematoxylin and eosin and gomori’s trichrome stain.
Gross anatomy of teeth and TMJ of adult dog
Our observations revealed the following:
Dental features
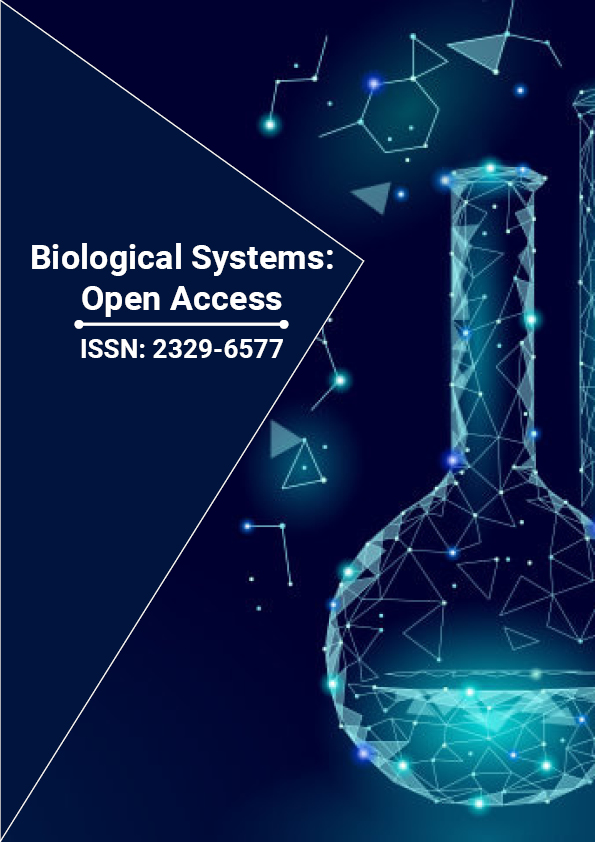
Teeth are large in size with the roots being much longer than the crowns, and the root trunk in premolars and molars is almost not present (Figure 1).
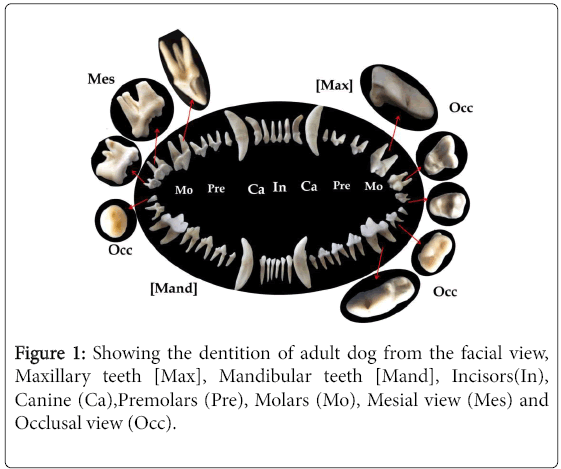
Figure 1: Showing the dentition of adult dog from the facial view, Maxillary teeth [Max], Mandibular teeth [Mand], Incisors(In), Canine (Ca),Premolars (Pre), Molars (Mo), Mesial view (Mes) and Occlusal view (Occ).
Incisors: Maxillary incisors are broad mesiodistally from the labial aspect, the 1st is the smallest and the shortest of all incisors, the crown is approximately one third the length of the root. The incisal surface is formed of three rounded elevations and the central elevation in the incisal surface that is elongated and presenting a close resemblance to canine cusp. The 2nd is similar to the first but slightly longer, while the 3rd resembles the canine but much smaller in size and its root is broad angular and curved distally to a great extend ending in a square apex (Figure 1).Mandibular incisors are thinner and longer than the maxillary incisors. They increase in length and width gradually from the first to the third incisor. The roots are straight and have very narrow apices (Figure 1).
Canines: They are the longest teeth in the arch; the crown is about three quarter the length of root in maxillary canine which is slightly longer and slightly more curved than the mandibular one. The root is broad mesiodistally and ends with a round blunt apex in both (Figure 1).
Premolars: Maxillary first premolar: It is the shortest and smallest of all maxillary teeth, the crown is very short occlusocervically but broad mesiodistally, and it has one small cusp pointed distally. It has one short root with a blunt apex. Maxillary second and third premolars: They are exactly of the same morphology with the third being slightly larger. The crown has two cusps one large mesial and a much smaller distal one separated by a deep groove. The crown surface is slightly convex on the facial surface and more concave on the palatal surface. They have two widely separated roots; one mesial and one distal, the distal root is wider cervically than the mesial one, and each taper apically to a blunt apex. There is almost no visible root trunk. Maxillary fourth premolar: It is the largest tooth in the maxillary arch, it is slightly wider mesially than distally, it has 2 cusps, the mesial one is wide and pointed, but the distal one is smaller and more flat, both separated by a short deep groove that ends with a large pit on the buccal surface of the crown. The facial surface is convex while the palatal is flat. It has three roots; 2 mesial and one distal, the mesiolingual one is the thinnest and the shortest while the distal is the broadest and the longest. Mandibular premolars: They are very similar to the maxillary ones except the fourth mandibular premolar, which is similar to the third mandibular premolar and not to the maxillary fourth premolar (Figure 1).
Molars: Maxillary first molar: The crown appears triangular from the occlusal view with the apex of the triangle pointing lingually, it contains three large cusps; two buccal and one lingual with a deep circular central fossa, the lingual cusp is subdivides into three smaller elevations; one mesial and two distal. The mesial surface of the crown is convex while the distal surface is concave. It has three roots two buccal and one lingual, the buccal roots are small, short, and have irregular rounded apices. The lingual root is the shortest and widest of them all and has a wide flat square apex (Figure 1). Maxillary second molar: It is the shortest tooth in the oral cavity. From the occlusal surface, it is very similar to the first molar but smaller in size. The distobuccal root is fused to the lingual root (Figure 1). Mandibular first molar: It is the largest tooth in the mandibular arch and it is very wide mesiodistally. From the facial view it has three cusps; with the middle being the largest, and the distal being the shortest, from the occlusal view there are five cusps, three on the mesial side and two on the distal separated from each other by a deep fossa. It has two roots similar in size, broad cervically and with almost no root trunk (Figure 1). Mandibular second molar: It is broad mesiodistally than buccolingually, with three cusps; two long mesial cusps and one short distal cusp, separated by a shallow circular fossa. It has two roots, the mesial is thin, and distal slightly thinker and both are curved distally (Figure 1). Mandibular third molar: It is very small tooth having a rounded crown with two very shallow circular fossae and no distinct cusps; it has only one short conical root (Figure 1).
Bony components of TMJ of adult dog and their relations to each other
The joint is located anteroir and slightly superior to the eustachian tube and Tymbanic bulla, bellow the posterior end of zygomatic arch (Figure 2A) the glynnoid fossa in which the condylar head articulates is oval in shape and directed mediolateraly (Figure 2B and 3A), it has a small rounded elvation on the posterior end called the retroarticular process ,and a flat smooth anterior and lateral ends(Figure 2A, 2B and 3A). The zygomatic arch is composed of two bones the zygomatic bone and the zygomatic process of the temporal bone. It covers the dorsal part of the coronoid process (Figure 2A). The Mandible is composed of two halves joind together by symphesis mentalis (Figure 3B) it has a long body which carries the teeth, a long rounded coronoid process that forms a shallow mandibular notch with the condyle which ends slightly above the occlusal surface of molars. There is a deep V-shaped depression on the ramus in which the masseter muscle is attatched called the massetertic fossa,the mandibular angle is proturuded backward and forms a wide acute angle with the condyle(Figure 2C).The condylar head is smooth, narrow antroposteriorly and wide mediolateraly. It is perpendicular to the occlusal plane of teeth and slightly angulated in relation to the coronoid process (Figure 3B).
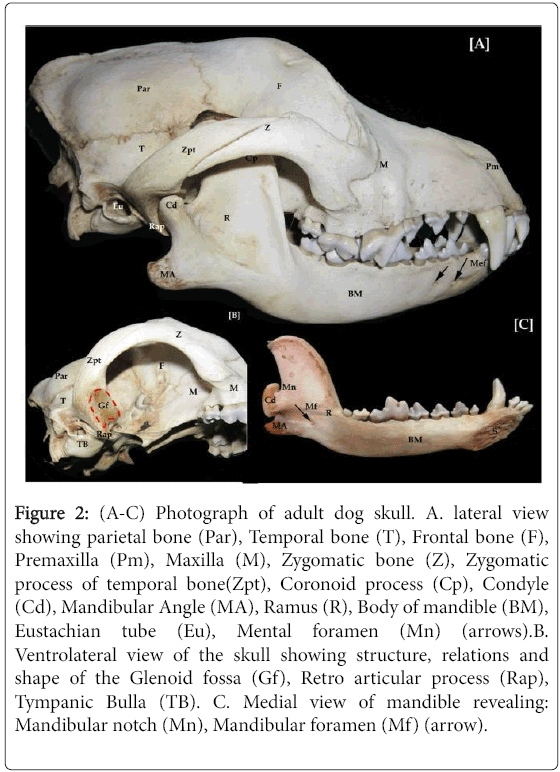
Figure 2: (A-C) Photograph of adult dog skull. A. lateral view showing parietal bone (Par), Temporal bone (T), Frontal bone (F), Premaxilla (Pm), Maxilla (M), Zygomatic bone (Z), Zygomatic process of temporal bone(Zpt), Coronoid process (Cp), Condyle (Cd), Mandibular Angle (MA), Ramus (R), Body of mandible (BM), Eustachian tube (Eu), Mental foramen (Mn) (arrows).B. Ventrolateral view of the skull showing structure, relations and shape of the Glenoid fossa (Gf), Retro articular process (Rap), Tympanic Bulla (TB). C. Medial view of mandible revealing: Mandibular notch (Mn), Mandibular foramen (Mf) (arrow).
Figure 3: (A, B) Photographs of the skull and mandible of adult dog. A. Ventral surface of skull showing, Premaxillary bone (Pm), Maxilla(M), Frontal bone (F), Zygomatic arch (Z), Temporal bone (T),Glenoid fossa (Gf), Tympanic bulla (TB). B. Dorsal surface of the mandible showing, Symphysis mentalis(S), Coronoid process (Cp), and Condyle (Cd).
Soft tissue components of TMJ of adult dog
The skin and subcutaneous tissue was removed, the masseter muscle which was extending from the zygomatic arch to the lower border and angle of mandible is seen (Figure 4A). The zygomatic arch, condylar head, and mandibular angle can be seen clearly after removing that layer of masseter muscle (Figure 4B).The condylar head was located bellow the posterior end of Zygomatic arch above the angle of mandible in front of the masseteric fossa (Figure 4C), when the condyle was slightly detached from its place the glenoid fossa of the Zygomatic arch could be clearly seen (Figure 4D).The joint is fully covered by the articulating capsule which is hard, thin fibrous tissue attached to the zygomatic arch and the head of the condyle (Figure 5A and 5B). Glenoid fossa appeared smooth with a retroarticular process in the posterior border and no eminence anteriorly (Figure 5C). The articular disc is attached to the lateral pterygoid muscle anterior-medially. It is oval in shape and has a thick periphery and thin central portion (Figure 5D). The articular disc divides the TMJ cavity into upper and lower joint cavities. Posteriorly it is attached to the retroarticular process and neck of condyle. Anteriorly, it is attached to anterior border of glenoid fossa and condylar neck (Figure 6A and 6B).
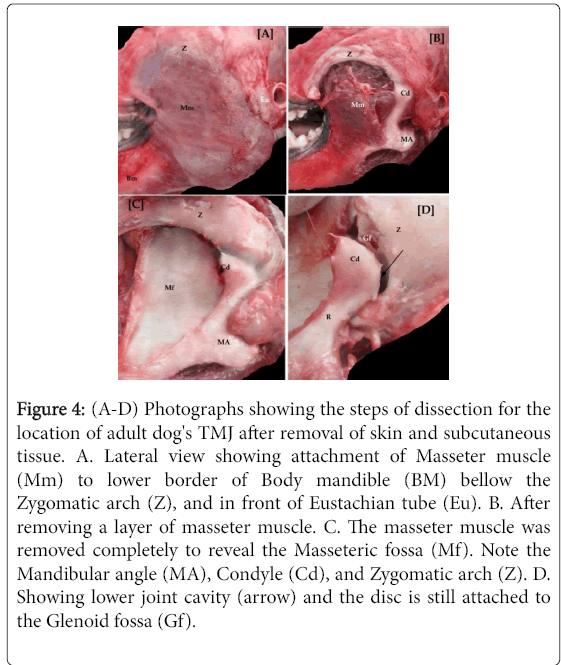
Figure 4: (A-D) Photographs showing the steps of dissection for the location of adult dog's TMJ after removal of skin and subcutaneous tissue. A. Lateral view showing attachment of Masseter muscle (Mm) to lower border of Body mandible (BM) bellow the Zygomatic arch (Z), and in front of Eustachian tube (Eu). B. After removing a layer of masseter muscle. C. The masseter muscle was removed completely to reveal the Masseteric fossa (Mf). Note the Mandibular angle (MA), Condyle (Cd), and Zygomatic arch (Z). D. Showing lower joint cavity (arrow) and the disc is still attached to the Glenoid fossa (Gf).
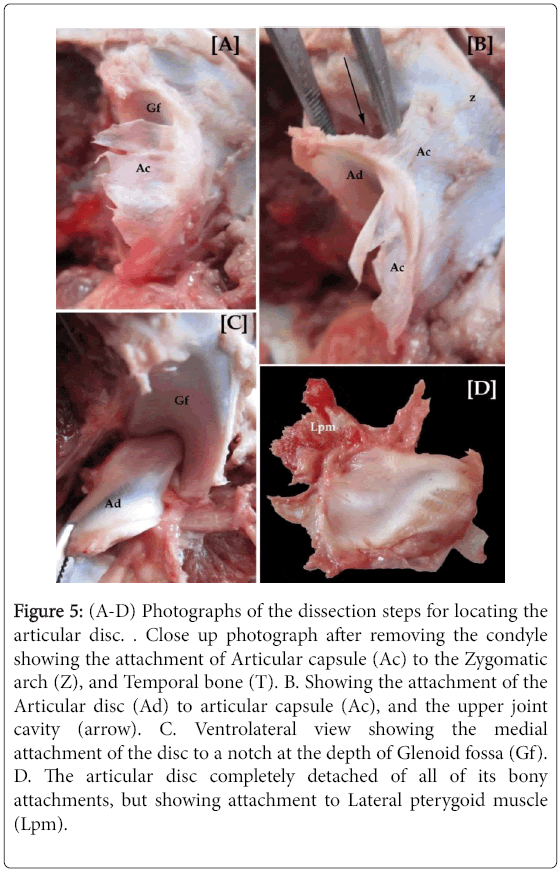
Figure 5: (A-D) Photographs of the dissection steps for locating the articular disc. . Close up photograph after removing the condyle showing the attachment of Articular capsule (Ac) to the Zygomatic arch (Z), and Temporal bone (T). B. Showing the attachment of the Articular disc (Ad) to articular capsule (Ac), and the upper joint cavity (arrow). C. Ventrolateral view showing the medial attachment of the disc to a notch at the depth of Glenoid fossa (Gf). D. The articular disc completely detached of all of its bony attachments, but showing attachment to Lateral pterygoid muscle (Lpm).
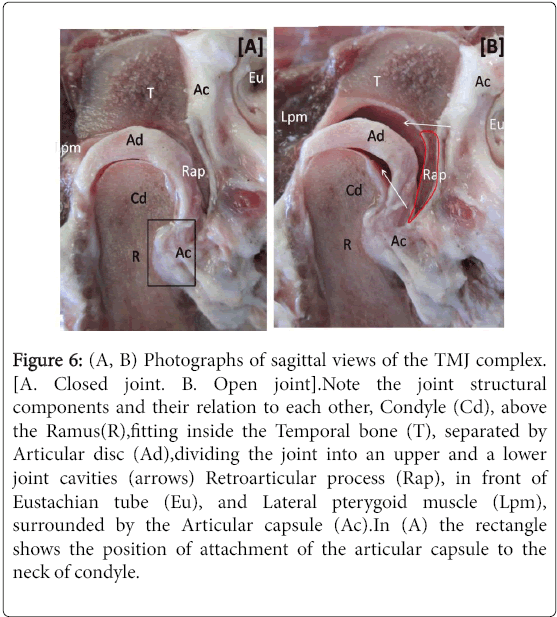
Figure 6: (A, B) Photographs of sagittal views of the TMJ complex. [A. Closed joint. B. Open joint].Note the joint structural components and their relation to each other, Condyle (Cd), above the Ramus(R),fitting inside the Temporal bone (T), separated by Articular disc (Ad),dividing the joint into an upper and a lower joint cavities (arrows) Retroarticular process (Rap), in front of Eustachian tube (Eu), and Lateral pterygoid muscle (Lpm), surrounded by the Articular capsule (Ac).In (A) the rectangle shows the position of attachment of the articular capsule to the neck of condyle.
Histological structure of TMJ of adult dog: Mandibular condyle
Mandibular condyle
The articular surface of adult dog's condyle is covered by a broad fibrous layer, followed by a layer of fibroblast-like proliferative cells (cell-rich zone) where the cells run mostly parallel to the articular surface. The third layer mostly exhibited fibrocartilaginous character followed by a narrow zone of hypertrophied chondrocytes that could not be traced in all sections followed by the zone of cartilaginous maturation. Higher magnification of the fibrous layer revealed the presence of so many capillaries filled with red blood cells and found at the different depths of this layer (Figure 8C and 8D).The condylar head showed little or no cortical bone and the condylar trabeculae appeared fine, numerous, gradually increasing in size toward the center, and roughly perpendicular to the condylar surface both in sagittal and coronal sections (Figure 7A, 8C and 8D).
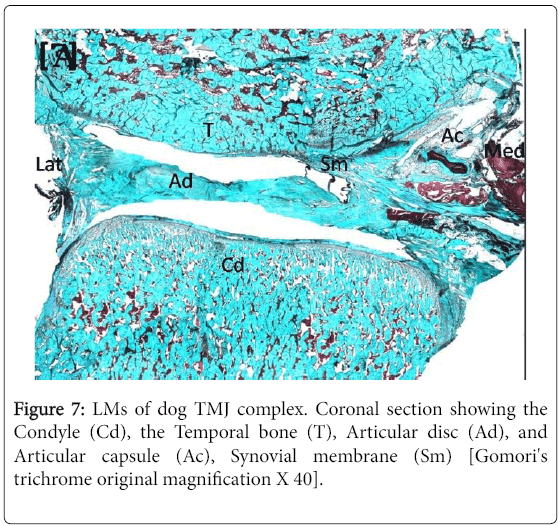
Figure 7: LMs of dog TMJ complex. Coronal section showing the Condyle (Cd), the Temporal bone (T), Articular disc (Ad), and Articular capsule (Ac), Synovial membrane (Sm) [Gomori's trichrome original magnification X 40].
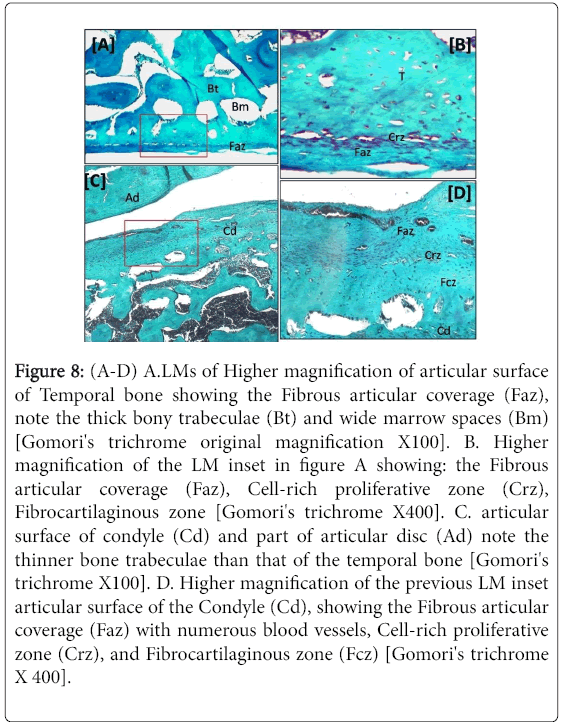
Figure 8: (A-D) A.LMs of Higher magnification of articular surface of Temporal bone showing the Fibrous articular coverage (Faz), note the thick bony trabeculae (Bt) and wide marrow spaces (Bm) [Gomori's trichrome original magnification X100]. B. Higher magnification of the LM inset in figure A showing: the Fibrous articular coverage (Faz), Cell-rich proliferative zone (Crz), Fibrocartilaginous zone [Gomori's trichrome X400]. C. articular surface of condyle (Cd) and part of articular disc (Ad) note the thinner bone trabeculae than that of the temporal bone [Gomori's trichrome X100]. D. Higher magnification of the previous LM inset articular surface of the Condyle (Cd), showing the Fibrous articular coverage (Faz) with numerous blood vessels, Cell-rich proliferative zone (Crz), and Fibrocartilaginous zone (Fcz) [Gomori's trichrome X 400].
Temporal bone
The surface coverings of the articular temporal bone showed no obvious regional variation. The fibrous coverage appeared slightly thinner than that of condyle and followed by a layer of high-density fibroblast-like cells (Cell-rich proliferative zone), the fibrocartilaginous layer is not distinct as the condyle (Figure 8A and 8B).The temporal bone had a thin cortex, large thick trabeculae randomly arranged (Figure 8A).
Articular disc
The disc appeared as a dense, fibrous structure. Anteriorly the disc splits into two bands, the upper band attaches to the temporal bone, and the lower one attached to the condylar head, in between these two bands, muscles fibers of lateral pterygoid muscle are inserted into the disc. Posteriorly, the disc is divided into inferior and superior lamellae. The inferior lamella is thin, extended from fibrous disc and covers the posterior surface of head of condyle. Laterally, the disc expands into a massive retrodiscal pad of fibrous tissue with adipose cells and blood vessels (Figure 7A and 9F).It has a thin central avascular part and thicker vascular peripheral parts especially the posterior part (Figure 9A-9C).
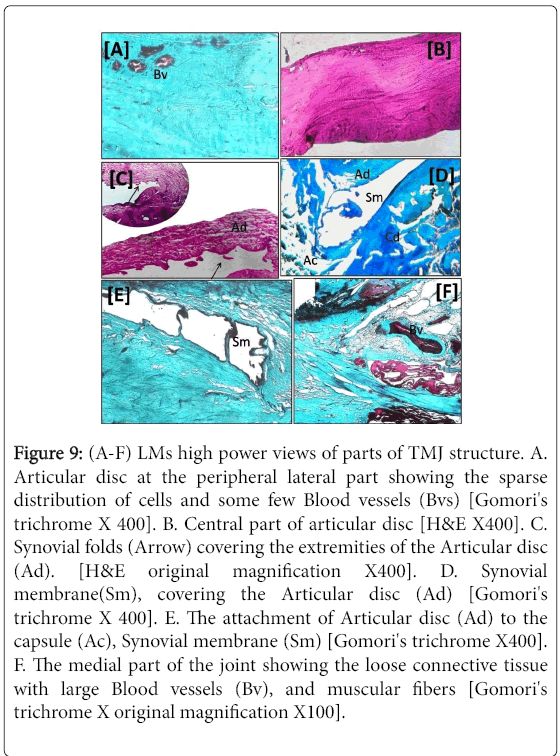
Figure 9: (A-F) LMs high power views of parts of TMJ structure. A. Articular disc at the peripheral lateral part showing the sparse distribution of cells and some few Blood vessels (Bvs) [Gomori's trichrome X 400]. B. Central part of articular disc [H&E X400]. C. Synovial folds (Arrow) covering the extremities of the Articular disc (Ad). [H&E original magnification X400]. D. Synovial membrane(Sm), covering the Articular disc (Ad) [Gomori's trichrome X 400]. E. The attachment of Articular disc (Ad) to the capsule (Ac), Synovial membrane (Sm) [Gomori's trichrome X400]. F. The medial part of the joint showing the loose connective tissue with large Blood vessels (Bv), and muscular fibers [Gomori's trichrome X original magnification X100].
Articular capsule
The TMJ capsule appeared loose collagenous membrane that attaches to the borders of the articular surfaces. This attachment enlarges posteriorly at the temporal and condylar divisions of the retrodiscal tissue. The anterior part of the capsule could also be followed in association with the attachment of lateral pterygoid muscle. Synovial membrane folds could be traced at the lateral and medial extremities of the disc overlying a strand rich in fat cells exhibited rich fat cells of adipose tissue (Figure 9C-9E).A Small to medium vessels could be frequent traced in the loose connective tissue anterior and lateral to the TMJ capsule (Figure 9F).
The use of experimental animals in research has contributed massively in medical advance for human health, it aided in testing of antibiotics, dialysis development, organ transplantation, vaccinations, chemotherapy, bypass surgery and joint replacement, which allowed us to live longer, healthier, and enjoying happier lives [23]. In the description of teeth, hard and soft anatomical components of TMJ as well as the histological of that joint in the experimental animals studied, we relied on and were guided by scientific information provided in universal documented literature [21,24-28]. Regarding the animal used in this study we could display, compare, and contrast the results we observed in the following points:
Dentition
Dog and human dentitions are diphyodont that has two sets of teeth (deciduous and permanent) [29]. They have ?brachydont or low-crowned teeth. This form and structure of tooth consists of a crown that shows above the gum line, a smaller neck at the gum line, and a deep root tied to the jawbone [30].
Teeth
Our findings of the anatomy and morphology of dog’s teeth correlated well with all of the description mentioned in the dental literature. The teeth of a dog are adapted for cutting meat and breaking bones. At the front of the skull are the small incisors that are used for nipping small pieces of meat from close to bones. The long strong pointed teeth behind the incisors are the canines, which are used for stabbing and killing prey. These teeth are also used as a display to threaten other dogs. The broader pointed teeth behind the canines are the premolars and molars, which are used for holding, cutting, shearing meat and for crushing bones. The largest of these teeth are known as carnassials, which work together to slice up meat like a pair of scissors [31,32]. The teeth of man are the result of a process of reduction and adaptation. As compared to most animal dentitions, the human teeth are deficient in number and in structure. This relative deficiency of the human teeth is associated with an advanced development of the brain: man has learned to use tools and weapons and to cook his food, and thus his teeth are no longer of vital importance to him. Some of the characteristics distinguishing the human from other mammalian dentitions are the fact that in man all teeth are in contact with each other and that all teeth erupt to the same level while in most animals some teeth are longer than others [31]. The dental arches are horseshoe in shape, with no diastema between teeth in both dentitions. While the dental arches in dogs are V-shaped and there is a small diastema between the third incisor and canine in upper arch and between canine and first premolar in lower arch.
Alveolar bone, zygomatic arch and temporal bone
In dog and man the zygomatic arch is made of two bones which are the zygomatic processes of both frontal and temporal bones [33,34].
Mandible
In our study, we noticed that mandibular suture of dog is firm. However for humans this suture is completely fused reflecting an important point of variation among animals on one side and between animals and man on the other side. The human mandible consists of a horseshoe-shaped body and a pair of rami. The body is divided into an upper alveolar part and the lower base. The ramus is smooth with no masseteric fossa and ends above in two processes-the coronoid anteriorly and the articular condyle posteriorly. Between them is a notch-the sigmoid notch. The shape of the mandibular angle of dogs is more prominent than man. [35,36]
Temporomandibular joint
The temporomandibular joint is critical for normal mouth function, and plays a role in chewing, swallowing, speaking, oral health, and nutrition. The TMJ is unique to mammals, but among different mammalian groups, its morphology and function vary enormously. Practicality dictates that animal models will not be the closest mimics of the human condition. Currently, the most used species are rats, rabbits, pigs, and ruminant ungulates. Each has distinctive TMJ adaptations [37]. Our observation confirmed this statement since we found that the anatomical structure of dog’s TMJ are different mainly in the shape and direction of both of the glenoid fossa and condyle and both are different from those of human. TMJ of dogs is a plain hinge joint that permits only opening and closing movement without lateral excursion, there is little or no actual mastication of food. The condyle and the mandibular fossa are elongated laterally and provide a strong hinge joint [31]. The TMJ of man is a modified synovial joint divided by an articular disk it allows hinge and sliding movements [25].
Mandibular condyle
Dog's condyle is cylindrical and has an inferior inclination medially. The long axes of the two condyles are directed at right angle to the midsagittal plane. The articular surface of the condyle could be divided into two parts, one horizontal on the superio-anterior part and one on the medial side of the posterior part [38]. Man's condyle is ovoid with the anteroposterior dimension being about half the mediolateral dimension. The long axis of the condyle is not at right angle to the ramus but diverged posterolaterally [25].
Temporal bone and the glenoid fossa
The mandibular fossa of dog is located mediolaterally, at the base of the zygomatic arc and well-defined retroarticular process is found caudal to it [34]. While in humans, the mandibular fossa is located on the inferior aspect of the temporal bone [24]. It is composed of an anterior part and a posterior part. Anterior part is in the form of eminence while posterior part is in the form of a depression or cavity in inferior part of temporal bone C) Disc: During dissection of TMJ, the articular disc of dog appeared thin, oval. The human TMJ the disk has a bow-tie-shaped biconcave morphology. The anterior and posterior ridges of the disk are longer in the mediolateral than in the anteroposterior dimension. The smaller anterior band attaches to the articular eminence, condylar head, and joint capsule. The posterior band blends with the bilaminar zone and the capsule. The bilaminar zone is residing in the retrodiscal space of the mandibular fossa and attaching to the condyle and temporal bone [39].
Capsule
In Dog's the TMJ was surrounded by a capsule. The capsule stretches from the edge of the mandibular fossa to the neck of the mandible, proximal to the pterygoid fovea, and envelops the articular eminence [40]. Humans capsule is a thin, slack cuff that does not limit mandibular movements and is too weak to provide much support for the joint. It is attached to the mandibular fossa and to the neck of condyle [25].
Histological study
Generally, in histological sections, the TMJ is composed of different tissues that include the condylar head, mandibular fossa, fibrocartilaginous disc, and fibrous capsule. [18,24,25] Based on the results of our study it is possible to say that, with regard to the histological features, there is a great similarity between dog’s, and human’s TMJ.
Bony components
Four main layers cover the articular surface of temporal bone as well as of the condyle. The first layer is a fibrous layer, in puppies, there was no obvious difference to that of human. The second layer is the cell-rich proliferative zone that showed no significant differences in all specimens. The third layer is consists of randomly arranged cartilage cells embedded in fibrous tissue forming the fibrocartilaginous zone. The final layer is the calcified cartilage zone, which also showed no remarkable differences.
Soft tissue components
There is an interposed fibrocartilaginous disc of biconcave morphology between the bony components. The structure and shape of the disc in dogs is similar to that of the human one [41]. No difference in the structure of capsule and synovial membrane from the human’s joint.