Research Article - (2017) Volume 6, Issue 1
By their behavior, human beings either succeed in achieving social integration or reveal the symptoms of some pathology. Objective: To determine family characteristics of schoolchildren with conduct disorders (CD). Methods: Prospective transversal study, with a descriptive and analytical scope, carried out from June 10th to July 12th 2013. The sample is made up of 235 schoolchildren registered for the 2012/2013 academic year in schools in Parakou. Parent-child relations were evaluated using the parental acceptance and rejection scale of Rohner and Khaleque in several dimensions. Results: Of the 235 schoolchildren considered, 44 had an exclusive CD, giving a prevalence rate of 18.7%. Slight CD stood at 38.6% while severe cases stood at 9.1%; sex-ratio for CD was 1.31; 40.9% of the children presenting these disorders were aged 10 years. 38.6% of them had made satisfactory progress in school; 15.9% and 13.6% of these children with CD “almost never” received any affection from their fathers and mothers respectively. None of the concerned children was “almost never” a subject of hostility-aggression. When indifference-neglect was at the least, we found 59.1% for the father and 56.8% for the mother. The “almost never” of undifferentiated rejection from the mother did not bring about any case of CD. Family communication was bad for 80.6% of sane children and 95.4% of children with CD. CD was correlated with lay private/confessional school (p=0.042). Conclusion: In our study, the attachment scheme for children with conduct disorders seemed rather disorganized. Globally, mothers seemed to have left a negative sentiment. CD occurs in specific environmental and family bases. There is a need for further studies and the development of appropriate strategies for effective prevention.
Keywords: School child; Conduct disorder; Parent; Affective dimension; Hostile dimension
Depending on their behavior, human beings more or less succeed to achieve social integration and to receive either a positive or a negative sanction from the society which generally observes, interprets and assesses their behavior right from childhood. In children, conduct disorder is “a set of observable and stratified reactions which show the child’s disorganization in several areas of life (personal, family, school and social life as a whole)…” [1]. Its manifestations include violence and aggressiveness towards self, others or even animals and objects. Clinically, conduct disorders (CD), attention deficit disorders with or without hyperactivity (ADHD) and oppositional defiant disorder (ODD) with provocation are close to the above definition. CD is often in co-morbidity with ADHD and is said to be a step towards ODD [2]. Conduct disorder can be considered as “a set of behavioral patterns which out rightly flout the fundamental rights of other persons and social norms or rules corresponding to the age of the subject” [3].
DSM IV classified CD into four main categories [4]: aggression to people and animals (criteria A1-A7), destruction or damage of property (material) without physical aggression (criteria A8-A9), deceitfulness or theft (criteria A10-A12) and serious violation of established rules (criteria A13-A15). In Africa, studies show a prevalence of ADHD situated between 5.4% and 8.7% for school children [5,6]. CD is often in co-morbidity with ADHD and constitutes a step towards TOD [2]. Neglected and rejected children and those suffering from parental indifference are more at risk as concerns the adoption of aggressive and antisocial behavior, or even violence in adulthood [7]. The number of condemned and imprisoned minors in Benin has grown from 64 in 2005 to 154 in 2009, representing 250% increase [8]. Family context, social life conditions and environmental factors are likely to influence development and persistence of CD in children and teenagers [3]. Postpartum maternal depression constitutes an obvious risk of conduct disorder in children [9], especially due to the hostile and coercive behavior of the depressed mother [10]. Family context is particularly implicated in CD and child delinquency [11]. There exists a link between the presence of CD in the child and the antisocial attitude of the parents [12,13]. Considering the above, we decided to embark on a study of the prevalence of CD in a town in northern Benin, notably amongst schoolchildren and its links with family characteristics.
Type of study, sampling and sample
It was a prospective transversal study, with a descriptive and analytical scope, carried out in the town of Parakou in the north of Benin. This town shelters populations from diverse backgrounds and has two educational zones, with 240 government and private schools. For the 2012-2013 academic years, there were 59,337 school children.
To determine the study sample, two strata for the government schools and two for the private schools were drawn at random from each zone in function of enrolment, making a total of four lots for the two zones.
The size of the sample was calculated using SCWARTZ’S formula [14]:
For a confidence level of 95%, Z=1.96; the prevalence, p obtained is 8.7% while the error margin, i=5% (0.05). Following the STEPS method of the WHO, k=1.5. Using this formula, the gross sample size obtained was N=183. With an expectation of 10%, the adjusted sample size was 202. However, taking into account the risk of questionnaires that might be poorly handled; we rounded up the number of school children to 300.
Only pupils of the CE2 to CM2 classes present in school on the day of the study were taken into consideration (classes four to six of the primary school cycle), the reason being that they were mature enough to quite easily understand the questions they were asked.
The study lasted for a period of one month, from 10th June to 12th July 2013. At the end of the study, 235 exploitable questionnaires were obtained from the 300 that were served, giving an achievement rate of 78.3%.
Conduct of the study
Every chosen pupil received a copy of the questionnaire. They were then asked to provide an answer to each of the questions after following the explanation from the person carrying out the study. The administration of the questionnaire took about 90 min, while the answers to the questions were noted. Next, the parents were invited for a session during which they were going to answer their own questionnaire and sign (or thumbprint) the consent request forms after an explanation of the process.
The various teachers, being the main advisors of the pupils, also answered to a questionnaire each.
Research instruments and variables studied
We used observation and interview, together with interview guides and questionnaires, other criteria and fixing mechanisms according to the chosen scale. The research instruments were questionnaires, DSM IV criteria for diagnosis and an adaptation of the parent-child relationship to the scale, the 2005 version of the Perceived Parental Acceptance and Rejection Theory of Rohner et al. [15].
This scale is aimed to evaluate the perception of the respondents on parental acceptance and rejection of children. It comprises four sub-scales: warmth-affection, hostility-aggression, indifference-neglect and undifferentiated rejection. Each item is evaluated with a score of four modalities which go from “almost always true” to “almost always false”. This scale is quite common in psychometric questionnaires and can be likened to Likert’s judgment scale, used in social and clinical psychology and in conducting opinion polls. The Parental Acceptance and rejection scale enables the respondents to express and balance up their degree of agreement or disagreement with the proposed opinions or points [16].
The score used in this study does not allow for neutrality. For each response, there is a possibility of attributing a score which enables an assessment of the given dimensions. The interviewers, all of them medical students at the end of their initial training cycle were trained on those aspects of the DSM IV concerning the diagnosis of CD and on the Parental Acceptance and Rejection Scale of Rohner and Khaleque.
In addition to the scores of the scale and the number of DSM diagnosis criteria, the study also took note of the factors linked to the degree of seriousness of CD in schoolchildren.
Variables examined in the study
Conduct disorder: Conduct disorder in children constitutes the dependent variable. The diagnosis of these disorders was carried out based on the DSM IV criteria. The respondents were divided into two groups: children with CD and sane children; we then calculated the prevalence rate and evaluated the severity of CD. The degree of severity of CD was evaluated using the same DSM IV criteria. This is a qualitative variable which was categorized following the number of symptoms observed. CD was considered light when 3-6 symptoms were observed, average with 7-9 symptoms and severe when there were more than 9 symptoms. The sex and age of the children at the time of the study, as well as the age at the beginning of the CD, were noted. The parent-child relationship was evaluated using the chosen scale: the “parental acceptance and rejection scale” of Rohner and Khaleque. For a better understanding, the questions were adapted and explained to the pupils in their native languages. The “warmth-affection” subscale describes the parent-child relationship in which the parent is viewed by the respondent as one who provides love and affection without necessarily making some very significant gestures. According to the respondents, an accepting parent is one who “generally loves the child, approves of its personality and pays attention to its activities and wellbeing”. The score was attributed as follows: almost always=4, sometimes=3, rarely=2, almost never=1. The greater the score in this subscale, the better the warmth-affection dimension of the parentchild relationship. The “hostility-aggression” subscale translates the case where the parent is viewed by the respondent as “angry, bitter and irritated with the child (perceived hostility) or trying to harm the child physically or even verbally (perceived aggression)”.
The “indifference-neglect” subscale evaluates the case where the respondent views the parent as “being uninterested and unconcerned by the child and his activities, paying little attention to the child and spending very little time with him”. The “undifferentiated rejection” subscale evaluates the situation where the respondent considers the parent as “being absent and considerably missing out on providing the child with warmth and affection”. The scoring scheme is the same: the lesser the score, the better the parent-child relationship within the hostility-aggression, indifference-neglect and undifferentiated rejection subscales. The evaluation of communication within the families was based on the ideas expressed by the responding children.
Socio-economic standard of parents: Given that the parents were generally quite reticent to declare their salaries and that a number of them were into informal activities and liberal professions and thus couldn’t quantify their periodic revenues, we took note of the money given to the children for their snacks and the type of school they attended as a measure of the socio-economic standard of the parents. The variable was explored using an ordinary questionnaire. Money given to the children for their snacks is that which enables them to buy some breakfast and/or lunch during break. The pupils do not always take their breakfast in the house: a number of parents and guardians give them some cash to buy it in school or along the way from vendors who propose several kinds of dishes. The term “pocket money” normally designates an amount given to children by their parents or guardians to enable them take care of their personal needs and comfort, out of the normal meals (breakfast, lunch, supper). In everyday usage however, “pocket money” or “morning allowance” is often used to designate the cash given to children for snacks.
Other characteristics: The question of cleansing rituals carried out to ward off bad omens was addressed. In Beninese habits, cultures and traditions, there are a number of rituals performed by family members to symbolically seek for favor and good luck or to ward off evil omen from a child. It is thought that CD is a sign of bad omen and rituals are often performed to ward it off. The “couple’s relationship”, a variable which depends on the frankness and objectivity of the parents, was not tested in this study because several kinds of parents were encountered: polygamous parents, single parents, reconstituted couples and substitutive parents (guardians taking the place of parents).
Data treatment and analysis
The variables were treated using version 20 of the SPSS software for windows while for the most part, tables and figures were conceived in Word and Excel or conserved as exported from SPSS. The Kruskal Wallis test was used to compare the various groups. The significance threshold was fixed at 5% for this study.
Ethical considerations
A request for authorization to carry out the study was deposited at the divisional directorate of primary and secondary education for Borgou division where Parakou, the town of the study, is situated. The interview forms were filled in strict confidentiality for each pupil, anonymity was strictly respected concerning school and identity of the respondents. Schoolchildren who were found to be suffering significantly (from CD) during the study were directed to specialists for consultation.
Prevalence
Of the 235 schoolchildren whose returned forms were exploitable, 44 were identified as showing exclusive CD without ADHD (Table 1), giving a prevalence of 18.7% in schools within the town. It was decided to exclude the pupils who showed co-morbidity between CD and ADHD.
| n | % | |
|---|---|---|
| Child with conduct disorder (CD) | 44 | 18,7 |
| Child with CD and ADHD | 16 | 6,8 |
| Child with ADHD without CD | 15 | 6,4 |
| Child "sane" ( without ADHD and without CD) | 160 | 68,1 |
| Total | 235 | 100,0 |
CD and "sane": 44+160=204.
Table 1: Repartition des ecoliers dela population initiale denquete selon leur symptome.
The results considered in the rest of this paper take into account the group of children with CD and those who are sound, respectively comprised of 44 and 160 pupils, what gives a total of 204 from the 235 respondents (Table 1).
Degree of severity
Of the 44 schoolchildren with CD according to the DSM IV criteria, 17 were found to have a slight condition, representing 38.6%; 23 had an average condition representing 52.3% and 4 had a severe CD, giving 9.1%.
Sex and age
Of the initial sample population, 48.5% were males (n= 114) while 51.5% were females (n= 121) with the M/F sex ratio being 0.94.
Of the group of 44 pupils with exclusive CD, there were 25 boys, giving 56.8%, and 19 girls representing 43.2%. The M/F sex ratio for children with CD was 1.31.
Of the 204 respondents finally retained, pupils with CD were divided into 25 boys representing 24.5% and 19 girls giving 18.6%, with p= 0.307.
At the time of the study, the age range of the initial population of respondents was 8 to 15 years, with an average of 10.7 ± 1.5 years. Amongst the children identified with CD, 40.9% were 10 years of age while 20.5% were 11 years, as against 28.7% and 24.8% respectively for the sound children. A comparison of the two groups in function of age using the Kruskal-Wallis test gives p=0.016 (Figure 1).
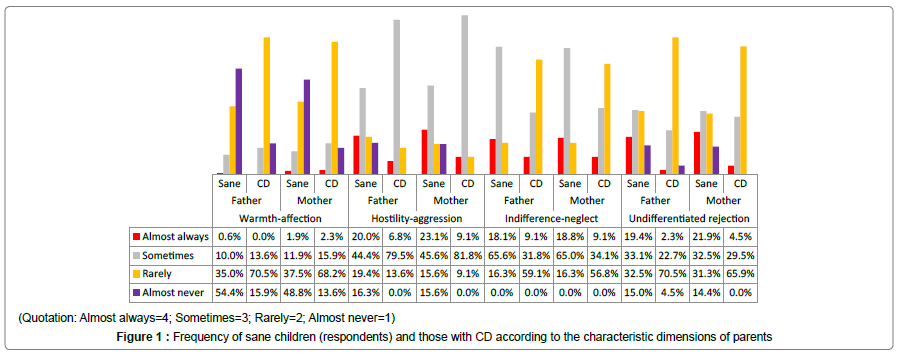
Figure 1: Frequency of sane children (respondents) and those with CD according to the characteristic dimensions of parents
In the studied sample, 92.3% of cases of CD started manifesting before the age of 10 years while 7.7% showed up after that age; 95.7% of the boys with CD had it before the age of 10 years, which was the case for 87.5% of the girls. A comparison of the groups “age at start of CD (age of onset)” and “sex” yields p=0.237 (Table 2).
| Test | Sig. | Decision | ||
|---|---|---|---|---|
| 1 | The distribution of sex is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.074 | Retain the null hypothesis |
| 2 | The distribution of age is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.016 | Reject the null hypothesis |
| 3 | The distribution of age of onset of the disorder is the same across categories of Sex. | Independent-Samples Kruskal-Wallis Test | 0,237 | Retain the null hypothesis |
| 4 | The distribution of age of onset of the disorder is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.222 | Retain the null hypothesis |
| 5 | The distribution of classes warmth-affection of the father is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.000 | Reject the null hypothesis |
| 6 | The distribution of classes warmth-affection of the mother is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.000 | Reject the null hypothesis |
| 7 | The distribution of classes hostility-aggression of the father is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.353 | Retain the null hypothesis |
| 8 | The distribution of classes hostility-aggression of the mother is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.683 | Retain the null hypothesis |
| 9 | The distribution of classes indifference-neglect of the father is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.000 | Reject the null hypothesis |
| 10 | The distribution of classes indifference-neglect of the mother is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.000 | Reject the null hypothesis |
| 11 | The distribution of classes undifferentiated rejection of the father is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.017 | Reject the null hypothesis |
| 12 | The distribution of classes undifferentiated rejection of the mother is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0.025 | Reject the null hypothesis |
| 13 | The distribution of Family communication is the same across category of Conduct Disorder | Independent-Samples Kruskal-Wallis Test | 0.019 | Reject the null hypothesis |
| 14 | The distribution of Money for snacks is the same across categories of Degree of severity | Independent-Samples Kruskal-Wallis Test | 0,001 | Reject the null hypothesis |
Table 2: Hypothesis test summary.
Slight CD were existed at several ages, with peaks at 10 and 12 years (29.4%), average CD were most frequent at 10 years (56.5%) while the severe ones were mostly noted at 8 and 9 years (Figure 2). The Kruskal- Wallis test for the groups of variables “age at start of CD” and “severity of CD” yielded p=0.222 (Table 2).
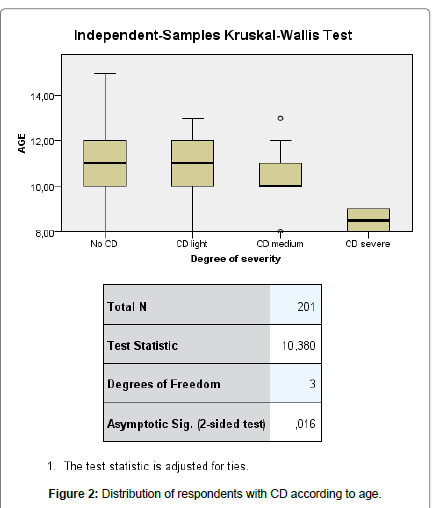
Figure 2: Distribution of respondents with CD according to age.
Affective and hostile behavioral attitudes of parents
The “warmth-affection” dimension: Children with CD, 15.9% declared that they “almost never” received warmth-affection from their fathers while 70.5% said they rarely received same, as against 54.4% and 35% respectively for sane children. From their mothers, 13.6% of the children with CD “almost never” received warmth-affection, as against 48.8% of sane children; 68.2% of them rarely received it as against 37.5% of sane children (Figure 1); p=0.000 for the warmth-affection dimension concerning both the fathers and mothers. The degree of severity of CD was correlated with the “warmth-affection” dimension (Table 2). The study revealed that 75% of severe CD occurs when there is “almost never” any warmth-affection from the father as well as the mother, while 95.7% occur when this warmth-affection is scarce. Where warmth-affection was “almost always” present from the mother, only 5.9% of slight CD were recorded and p=0.000 for the correlation.
The “hostility-aggression” dimension: This dimension enables an appreciation of the hostile and aggressive character of each parent towards the child. 79.5% of fathers and 81.8% of mothers were indexed by children with CD as belonging to the category “sometimes” with respect to this attitude. No child with CD placed their parents in the “almost never” category in this regard (Figure 1). Carrying out a comparison using the Kruskal-Wallis test for the “hostility-aggression” test yields p=0.353 for fathers and p=0.683 for mothers (Table 2).
The “indifference-neglect” dimension: CD occurred in equal proportions of 9.1% when the father and the mother were “almost always” Indifferent-negligent, while the proportions of sane children for the same score were 18.1% and 18.8% for the father and mother respectively. 59.1% of CD concerned the father while 56.8% were linked to the mother when “indifference-neglect” was not too pronounced. When the score of the dimension was “sometimes”, 65% of the children appeared sane. A comparison according to the degree of severity using the Kruskal-Wallis test for the indifference-neglect dimension yields p=0.000 for both the father and the mother (Table 2).
The “undifferentiated rejection” dimension: Considering the undifferentiated rejection dimension for each parent, both sane children and cases of CD were minimal for the extreme scores: “almost always” and “almost never”. On the scores “sometimes” and “rarely”, the proportion of sane children stood at 33.1% and 32.5% respectively for the fathers; 32.4% and 31.3% respectively for the mothers (Figure 1). In this dimension, the “almost never” was completely absent as concerns the mother, while for the father, the CD due to this score was slight and concerned just two cases from the 17 slight CD (11.8%). They were 50% of severe CD for the score “rarely” for both the father and the mother.
General attitude of parents towards the children
Maternal rejection (same like paternal rejection) did not lead to any severe or even medium case of CD. 11.9% of sane children and 23.5% of light CD cases suffered maternal rejection as against 11.3% and 23.5% respectively for paternal rejection. 68.1% and 67.5% of sane children had an acceptant father and mother, respectively. With an acceptant mother on the one hand and an acceptant father on the other hand, 20.6% of sane children and 25% of severe CD were recorded. The correlation between the general attitude of the father and the degree of severity of CD yields p= 0.086, while that between the mother’s general attitude and the degree of severity of CD yields p=0.054.
Family communication
Family communication was bad according to 80.6% of the sane children who responded, while 95.4% of the children with CD declared same. The correlation between the quality of communication and the degree of severity of the CD is shown in Figure 3 (p=0.019).
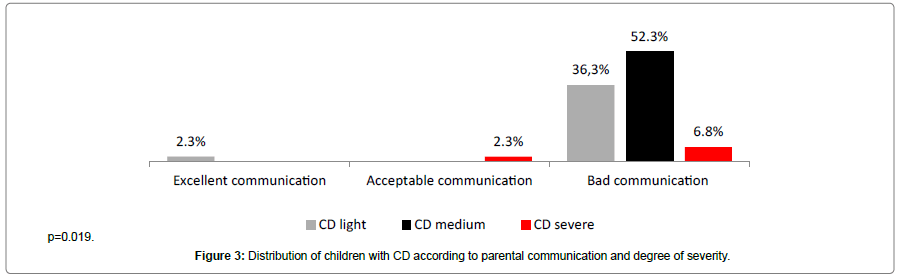
Figure 3: Distribution of children with CD according to parental communication and degree of severity.
Socioeconomic standard of parents
Money for snacks in school: To buy snacks in school, 57.2% of children with CD (Figure 4) had 50 francs CFA (less than a tenth of one US dollar) per day, against 29.2% of sane children; 46.1% of sane children were given 100 francs CFA as against 14.3% of children with CD. One of the sane children was given between 250 and 500 francs CFA, an amount none of the children with CD ever had. Those with CD had 50 to 100 francs CFA, with p=0.001.
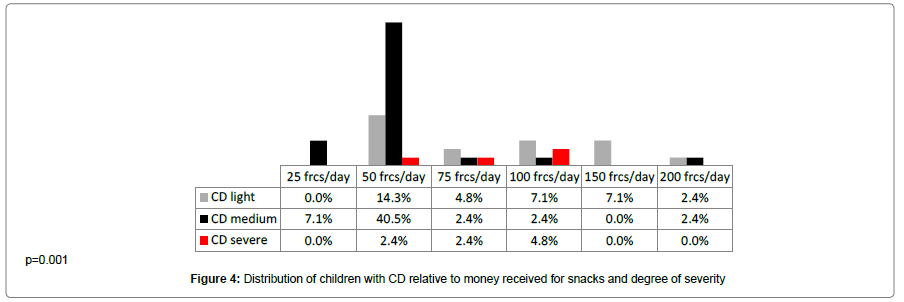
Figure 4: Distribution of children with CD relative to money received for snacks and degree of severity.
Type of school attended: It was found that 93.2% (n=41) of children with CD attended lay schools while 6.8% attended confessional schools. Within the 93.2% in lay schools, 84.1% attended government schools while 15.9% went to lay private schools. They were 79.4% of sane children in lay schools (76.3% in government schools and 3.1% in lay private schools) and 20.6% in confessional schools. The correlation between CD and type of school (lay/confessional) yields p=0.042.
The correlation between type of school and severity yields p=0.003. Cases of CD were only found in government and lay private schools, only 3 cases of CD (2 slight and one average) were found in confessional schools, making 6.8% of all the cases of CD.
Ritual ceremonies for warding off spells: In the event of CD affecting their children, many parents had turned to traditional practices and carried out one or more rituals usually performed to ward off spells in the hope of calming the situation, this was the case for 81.8% of children with CD (p=0.032).
Feel of parental love: The study revealed that 59.1% of children with CD thought that their fathers did not love them as against 26.3% for the sane children (p=0.000); 54.5% of children with CD said their mothers did not love them as against 25.6% for sane children (p=0.000).
Prevalence, sex and age
The prevalence rate of 18.7% for CD as revealed by this study appears quite high. Could it be because those who responded did so with a lot of ease? Several studies however point to the fact that male children of alcohol-dependent fathers are at a greater risk of developing CD and show a propensity to repeated alcohol consumption [17]. Behavioral disorders (oppositional defiance, attention deficit and physical aggression) could start rather precociously, at about 3 years of age for sons of alcohol-dependent fathers and then persist for a long time even if the child and father are separated [18], except if the separation is done for the purpose of protection. Given that Parakou is one of the towns in Benin where alcohol consumption is quite high [19], this high prevalence rate of CD can be explained otherwise. Indeed, postpartum maternal depression equally constitutes a serious risk factor for CD in children [9]. Depressed mothers are often unable to adequately cater for the needs of the child, what can explain the aggressive behavior developed by such kids both in early and late childhood [20]. According to our findings in this study (Table 2), the occurrence of CD is not statistically influenced by sex (p=0.074). However, the age at which it occurs differs according to sex: CD occurs in males at an earlier age than in females. The peak of 10-11 years observed in this study is apparently not a function of sex but of the population of the study.
Warmth, affection and communication dimensions
For children with CD, 2.3% of the mothers were said to have “almost always” been providing warmth-affection, whereas not a single father did same (Figure 1). For the group of parents “almost never” giving warmth-affection, the number of fathers was slightly more than that of fathers (13.6% and 15.9%). It appears that the mothers showed more affection and warmth towards the kids than fathers. Children with CD were more common in the group of kids whose parents scarcely ever showed them any warmth-affection: the occurrence was twice greater than in the case of sane children.
The study revealed that the number of sane children who never received any “warmth-affection” from their parents was more than 3 times greater than that of children with CD who faced the same issue (Figure 1). The correlation (Table 2) is statistically significant (p=0.000). It is possible that in the wake of the occurrence of CD, parents may have improved on their attitude as far as affection is concerned, in order to soothe the situation, or that children with CD are more demanding even in areas and issues where the sane ones show more restraint.
Here, there arises the problem of attachment and resilience. Children with CD are not quite satisfied when they receive a certain degree of “warmth-affection” from their parents, especially from their mothers. The most resilient of the children (about half of the sane children) who do not receive any affection from their parents behave as if they are already so sure that they will never receive it and as such, simply continue living their lives without that component. In this study, the attachment scheme for sane children appears to be swinging, while that for children with CD appears ambivalent or disorganized (insecure). Clinical studies have shown that an insecure attachment scheme is a risk factor for externalized trouble (TOP and CD) in children [2]. Pleux [21] affirmed that: “an individual needs love to be able to build up himself. Frustration however is also necessary. It needs to come to grips with reality”. According to the same author, parents have to “find and exercise the right authority”, mainly by advisedly saying no as “integrating the element of frustration” is “accepting the principle of reality” [22]. As for communication, the occurrence of CD increases by a factor of more than 40 when it is bad as compared to when it is good, with a statistically significant correlation (p=0.019). This result points to the fact that the quality of communication can be a predictive factor for CD (Figure 3).
Hostility dimension
Fathers and mothers had different profiles in the appreciation given to them concerning hostility-aggression. There is always a certain degree of hostility-aggression affecting children with CD. In the complete absence of hostility-aggression, no CD was noticed; while CD had a maximum occurrence when hostility-aggression was experienced “sometimes”. Severe cases of CD were divided between the scores “almost always” and “sometimes” for the two parents and “rarely” for the father. This could appear paradoxical. The hostility-aggression dimension has no influence on CD. Equally, the correlation between the severity of CD and the hostile attitude of parents is not significant.
In the “hostility-aggression” category, mothers seemed to have left greater negative feelings on the respondents than fathers. Does their role as primary educators not expose mothers to a tougher and more negative perception from the children? Fathers, given their rather distant attitude towards education within the home, globally appear less hostile and aggressive than mothers. However, the differences are not statistically significant (p=0.683 and 0.353). This result suggests that the absence of a person normally considered close (the mother) often leaves a greater impact than that of one who is usually not so close.
Indifference, neglect and rejection
The highest proportions of CD were found in children whose parents rarely showed “indifference-neglect” towards them, whereas sane children of such parents were relatively few. The lowest rates of CD were encountered amongst children whose parents were “almost always” indifferent and negligent (Figure 1). Either this dimension of parental behavior does not determine the occurrence of CD in a significant manner, or the children generally become less sensitive to the indifference-neglect of parents as they possibly begin counting on other resource persons. It could be that when CD begins, it becomes insensitive to the indifference-neglect attitude of parents (it does not improve even if the latter improves) and its evolution just continues. Since children with CD start facing difficulties in school earlier than those who are sane, their proportion in school gets quite reduced by the time their parents become “almost always” indifferent-negligent. An analysis of this hostile dimension of parents seems to suggest that they sometimes need to show a certain degree of indifference-neglect towards their children in order to increase the chances of the latter remaining sane. It is worthwhile to note that the evaluation of the various affective and hostile dimensions was done on the basis of the responses from the children who were interrogated. They might have overestimated the attitudes of their parents on these aspects; in any case, they are those living the experience (which is essential to their behavior).
Toupin et al. [23] in 2003 found that most of the children suffering from CD, especially those cases in which it starts quite early, generally also experience personal and family difficulties.
In our study, the undifferentiated rejection of parents appears to correlate with a high proportion of CD in the category “rarely”, coming both from the father and the mother.
Considering the “almost never indifferently rejecting” mother, there is no child with CD; it can be imagined that the absence of this hostile dimension for the mothers is a good founding factor for the children. However, there were only 14.4% of sane children with mothers in the same category “almost never indifferently rejecting”; p=0.025. The children are more demanding in the face of maternal rejection. Considering the fathers with the same characteristic (“almost never indifferently rejecting”), there were 4.5% of children with CD and 19.4% of sane children, with p=0.017. The analysis of this data shows a statistically significant correlation difference between undifferentiated rejection from the father and the child’s CD.
Socioeconomic standard
More than half of the children with CD received 50 francs CFA (a tenth of 1 US dollar) for snacks in school (Figure 4). This amount can only buy a third of a loaf of bread. This is obviously not enough to satisfy their hunger. Slightly less than half of the sane children received twice this amount. When CD starts, it is difficult for the situation to improve even when the triggering factors are removed.
The distribution of CD in function of the amount of money received for snacks particularly captured our attention. Indeed, the distribution seems to be guided by a certain law which starts at 125 francs and increases the proportion of disorder as the 25 francs mark is approached. The same law causes an exponential increase of the proportion of disorder as we go beyond 125 francs, but makes it to decrease as we move further away from that point. The number of children with CD (all were cases of light CD) amongst those receiving 150 francs as money for snacks was about four times greater than that of sane children. This observation suggests that there is an ideal amount with respect to which the school children do compare, and its difference with the amount received determines the occurrence of CD. The distribution is the same for both public and private schools. Severe cases of CD are encountered at 75 ± 25 francs. The correlation between CD and money for snacks gives p=0,001, which is an indication of the statistical significance of the variable “money given for snacks” on CD.
Moreover, it is in function of their socioeconomic standard that parents often choose the type of school which their children attend. There was a greater prevalence of CD in public schools as compared to the number of sane children, while the prevalence in private schools was quite reduced, especially in the confessional schools. Considering the private schools, there were more cases of CD in lay private schools, indicating that fewer sane children attended those schools. The category “lay/confessional” exerts a statistically significant influence on CD (p=0.042). Are children with CD or those showing signs of disorder sent away from confessional schools, or is it the intrinsic characteristics of the families of children with CD which prevent them from enrolling and remaining in confessional schools? It is known that the fee in confessional schools is generally high; poor parents cannot afford to send their children to such schools [23].
Appreciation of parental support and love
Brothers and sisters did not count at all for children with CD; father and mother did not count for much. Children with CD often turned to a friend as a first resort when in difficulty as opposed to sane children; they felt that their fathers did not love them (59.1% as against 26.3% for sane children). This suggests that children with CD have a feeling of affective deficiency which is twice that of sane children. Does this feeling favor or maintain CD?
Even though parents loved them, the emotional needs of children with CD are still not being met. Parents often did not display it clearly or appropriately.
It should be noted that a very vulnerable family environment often does not have the necessary resources to manage the behavioral difficulties of the child. This can contribute to the deterioration of parent-child relationships and the exacerbation of problems [24].
The severity of behavioral disorders is significantly associated to a majority of the functional dimensions of the family [25].
Cleansing rituals
Traditional initiation ceremonies give an early testimony of the child’s place and membership in his family or his community at large. It enables them to come to full knowledge of the ancestor who placed his seal on their entry into the world and/or their destiny. It is believed that these consecration rituals serve to boost each individual’s stability. With the development of foreign religions, these rituals are gradually being abandoned. Nevertheless, when difficulties arise, the parents begin to ask questions and often go back to traditional practices. This is the case with 81.8% of the families of children with CD (p=0.032).
CD and evolution
For some authors [26], it is necessary to worry, and this as soon as possible, since longitudinal studies have shown that children with several symptoms of CD are at a serious risk of having problems with social adaptation; physical, mental and reproductive health, together with problems while trying to integrate the job market [27-29] if the risk factors persist and no care is provided. As consequences, these authors cited failure in school, rejection from peers, consumption and abuse of alcohol and psychoactive substances, delinquency and risky sexual behavior. Depression, contemplation and even attempts at suicide are not rare.
It is essential to note that not all abnormal behavior necessarily leads to delinquency; also, is the society the toughest and at the same time the most clement of judges on matters of normal and abnormal behavior.
It is therefore important to know more about the CD, in order to be able, depending on the circumstances, to soften the diagnostic hypotheses and to initiate preventive measures and/or initiate a solid and adapted management for a better well-being of the patient and his entourage [30].
Conduct disorder in children arises in specific family and environmental conditions and often leaves negative residual traces on the ensuing adolescents and adults. It is thus necessary that other studies should be done, with the elaboration and use of strategies which are reliable and adapted to the socio-family and environmental context at large for an effective primary prevention if possible, or as the case may be, secondary or tertiary prevention.
