Research Article - (2015) Volume 4, Issue 2
Introduction: Hypothyroidism, metabolic syndrome and central obesity are common diseases known as the risk factors for atherosclerotic cardiovascular disease. The co-existence of thyroid dysfunction in obese patients might substantially increase the cardiovascular risk. The objective of the study was to evaluate the effect of hypothyroidism on the main cardiovascular risk factors in patients with obesity and cardiovascular syndrome.
Material and methods: In a cross-sectional clinical study we examined 202 patients with central obesity and metabolic syndrome (160 women, 42 men, aging 43 ± 13 yrs) with BMI ≥ 30 kg/m2 divided in two groups - 101 patients with subclinical or overt hypothyroidism (gr. A-hypot) and 101 eythyroid patients (gr B-eut), diagnosed by TSH, FT4,TPO-Ab. Laboratory assessment included: total cholesterol (TChol), HDL,LDL, triglycerides (3-glyc), serum glucose, standard oral glucose tolerance test (OGTT) and insulin resistance by Homeostasis Model Assessment of Insiline Resistance (HOMA-IR). Serum leptin and C-reactive proteins were estimated in 20 patients of each patients group and in a control group of 20 healthy persons with BMI <25 kg/m2. The supplementation Levothyroxine therapy was carried out of patients with overt and subclinial hypothyroidism.
Results: Both compared groups showed similar BMI (mean 37 kg/m2) and HOMA-IR value 3.1 and 3.15, respectively Mean TSH value was found 4-fold higher in gr. A than in gr. B. which significantly correlated with TChol, 3-glyc, CRP and serum leptin The prevalence of arterial hypertension (AH), diabetes type2 or impaired glucose tolerance (IGT) in gr A was 86% and 67% vs. 80% and 70% in gr B, respectively. Significant correlations were established between TSH, TChol, atherogenic lipoproteins, 3-glyc. in patients gr. A but not in gr B. The same parameters decreased significantly after adequate levothyroxin supplementation. The significant positive nonparametric correlations were found also between BMI, TSH, leptin and CRP (p<0.05).
Conclusion: Our data demonstrate that hypothyroidism significantly aggravates the lipid metabolisms in patients with obesity or MetS. These disturbances co-existing with higher prevalence of arterial hypertension, DM-T2 or IGT determine the substantially increased cardiovascular risk which correlated with increased insulin resistance, higher levels of leptin and CRP as a marker of chronic inflammation. Consequently clinicians shouid be particularly alert in the possibility of thyroid disfunction in obese patients.
Keywords: Hypothyroidism; Obesity; Cardiovascular risk; Lipids; Leptin
Obesity is one of the most important health risk of our time which is associated with an increased incidence of diabetes, dyslipidemia, kidney disease and cardiovascular disease [1,2]. The central obesity and metabolic syndrome are linked also to many endocrine abnormalities especially hypothyroidism which is established in up to 35-43% of patients in some series [3-5].
Evidence suggests that slight variations in thyroid function, even as indicated by tests that are within laboratory reference ranges, contribute to the development of regional obesity and the tendency to gain weight [6-9]. This is not surprising because the active thyroid hormone triiodothyronin (T3) regulates energy metabolism and thermogenesis, and plays a critical role in glucose and lipid metabolism, food intake and the oxidation of fatty acids. On the other hand, the onset of thyroid hormone deficiency, especially the subclinical form, may go undiagnosed in obese patients. Consequently, these patients will continue to gain weight and will develop a deranged lipid profile, thereby bringing the thyroid/obesity association to a full circle [10]. Some data show that co-morbidity of obesity and hypothyroidism appeared much more important risk factors for atherosclerotic cardiovascular disease mediated mainly by the accelerated effects of thyroid hormones on lipid metabolism and blood pressure [11].
The objective of the study was to compare some markers of the cardiovascular risk in subjects with obesity and metabolic syndrome with and without hypothyroidism.
In a cross-sectional study we examined 202 patients with visceral obesity –OB and metabolic syndrome - MetS (160 women, 42 men, aging 43 ± 13 yrs) with BMI ≥ 30 kg/m2, divided in two groups - 101 patients with spontaneous autoimmune hypothyroidism (gr. A) and 101 pts with a normal thyroid function - euthyroid (Gr B). The diagnosis of MetS was established according to the criteria of International Diabetic Federation (IDF) -2005 including 3 or more of following parameters:
1) Fasting blood sugar ≥ 6,1 mmol/L, impared glucose tolerance (IGT) or type 2 diabetes, 2) Arterial hypertension ≥ 140/90 mmHg, 3) Triglycerides ≥ 1,7 mmol/L, 4) HDL-C <1,0 mmol/L for men or <1,3 for women, 5) Visceral obesity: Waist circumference >102 cm for men or 88 cm for women or BMI ≥ 30 kg/m2 [12].
Hypothyroidism (Hypot) was confirmed by serum TSH >4.94 mIU/L (n. range 0.35–4.94 mIU/L) and FT4 (n. range 9-19.05 pmol/L) in two consecutive measurements. Most of the patients in gr. A had a normal FT4 (subclinical hypothyroidism) and only 12/101 revealed the overt Hypot (high TSH, low FT4). The adequate supplementation Levothyroxine (L-T4) therapy was carried out in 58 patients with overt or subclinical hypothyroidism.
Serum TSH, FT4 and insulin were estimated by chemiluminiscent microparticle immunoassay-CMIA, based on mouse monoclonal antibodies). Serum glucose-by hexokinase method, total cholesterol by enzymatic method (Trinder endpoint reaction), HDL and LDL– by direct enzymatic assay, triglycerides by colorometry. Serum leptin (ELISA, ref.r. 4.5 – 20.8 ng/ml) and C-reactive proteins (CRP) were estimated in 20 patients of each patients group and in a control group (20 healthy persons with BMI <25 kg/m2). All non diabetic patients performed Oral Glucose-Tolerance Test (OGTT) on 0-60-120 min. Insulin resistance (HOMA-IR) was calculated by Fasting plasma glucose level (mmol/L) X fasting insulin level, divided by 22,5 (normal value ≤ 2,5).
The statistics were processed using variation and frequency analysis, nonparametric, parametric and correlation analysis performed using SPSS for Windows 13.
No statistically significant differences there were between groups of hypothyroid and euthyroid OB/MetS patients (A and B groups) regarding to the number of cases, mean age, mean body weight and BMI. Mean BMI values corresponded to obesity of second degree-36.86% and 37.35, respectively (Table 1). These corresponded to the similar increased insulin resistance, expressed as HOMA-IR in both groups (mean values of 3.10 ± 2.4 and 3.15 ± 2.1 respectively).
| Patients | Gr A /Hypothyroid pts /n=101/ | Gr B/ Euthyroidpts /n=101/ | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Median | Mean | SD | Median | |
| AGE (years) | 39,47 | 39,00 | 12,39 | 42,00 | 41,20 | 13,01 |
| WEIGHT (kg) | 104,99 | 24,06 | 98,00 | 104,14 | 22,32 | 99,50 |
| BMI (kg/m2) | 36,86 | 6,53 | 35,45 | 37,35 | 6,60 | 35,00 |
Table 1: Mean anthropometric variables of OB/MetS patients with and without hypothyroidism.
The prevalence of AH was higher in hypothyroid than in euthyroid patients – 67.1% vs. 54.5%. It was not any significant difference in the prevalence of DM-type 2 and pre-diabetes but as might be expected the prevalence of arterial hypertension (AH) and diabetes type2 (DM-2) or prediabetes (impaired glucose tolerance IGT, IFG) were much higher in MetS than in OB patients in each compared group (Table 2).
| Subgroups | N | AH | DM-2 | IGT+IFG+IGT/IFG | Normal glucose tolerance |
|---|---|---|---|---|---|
| MetS+Hypot | 61 | 53/61 86% |
19/61 31% |
15+4+3=22/61 36% |
20/61 32% |
| OB+Hypot | 40 | 14/40 35% |
2/40 5% |
3+1+1=5/40 12% |
33/40 82% |
| MetS - euthyroid | 51 | 41/51 80,4% |
17 33,3% |
7+9+3=19/51 37% |
15/51 29% |
| OB - euthyroid | 50 | 14/50 28% |
1/50 2% |
2+2+1=5/50 10% |
44/50 88% |
Table 2: Frequency of arterial hypertension (AH), diabetes type 2 (DM-2) and prediabetes (impaired glucose tolerance - IGT, impaired fasting glucose - IFG or both - IGT + IFG) in patients with obesity OB /MetS with and without hypothyroidism
Statistically significant correlations (r=0.54, p<0.02) were found between BMI, serum TSH, Leptin and CRP.
Serum TSH means value was 4-fold higher in gr. A than in gr. B (p<0.001). Significant positive correlations (p<0.01) were established between TSH, T-Chol, 3-glyc in patient’s gr.A but not in gr B (Table 3, Figure 1-3). The same parameters decreased significantly after adequate L-T4 therapy of hypothyroidism (Figure 4).
| Patients | ТSH | Cholesterol | HDL | 3-glyc |
|---|---|---|---|---|
| groups | (mIU/l) | (mmol/l) | (mmol/l) | (mmol/l) |
| Gr. A (Hypothyroid) |
5,82±6,7 | * 5,58±0,99 | 1,21±0,25 | *1,79±1,09 |
| Gr. B (Euthyroid) |
1,70 ±0,82 | * 5,37±1,07 | 1,25±0,30 | *1,61±1,03 |
| P | <0.05 | >0,05 | <0,05 |
Table 3: Mean values and SD of TSH and biochemical variables in two compared groups of obese patients – with and without Hypothyroidism (*P<0.05).
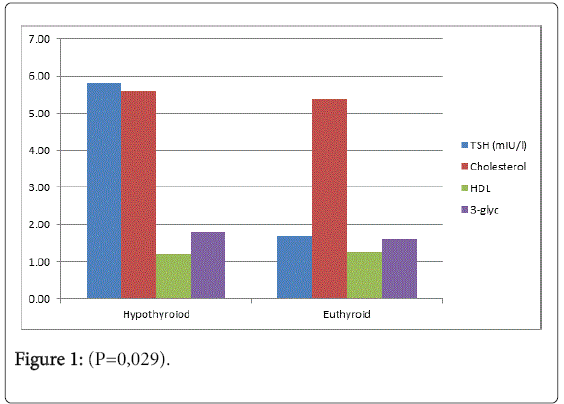
Figure 1: (P=0,029).
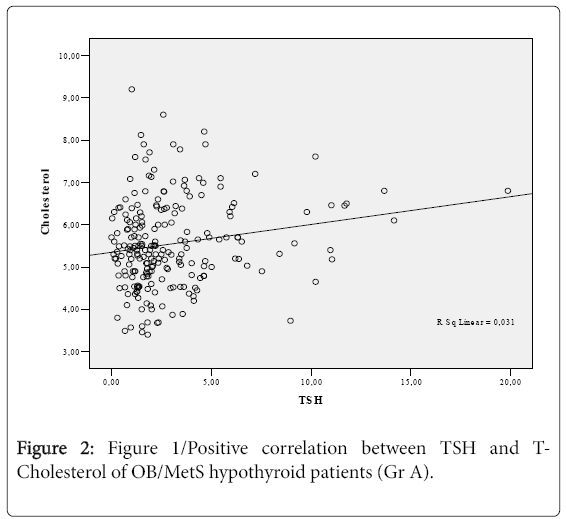
Figure 2: Figure 1/Positive correlation between TSH and TCholesterol of OB/MetS hypothyroid patients (Gr A).
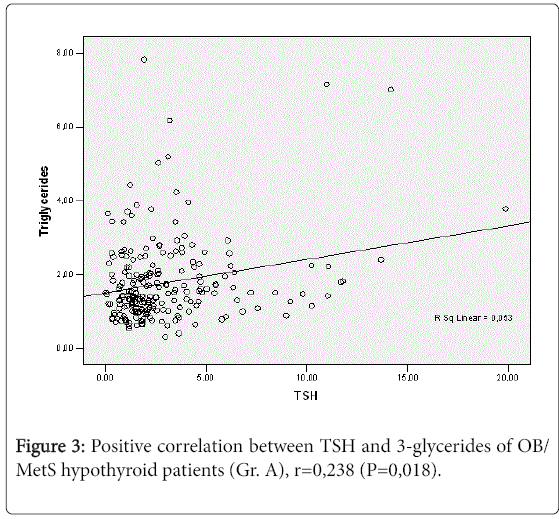
Figure 3: Positive correlation between TSH and 3-glycerides of OB/ MetS hypothyroid patients (Gr. A), r=0,238 (P=0,018).
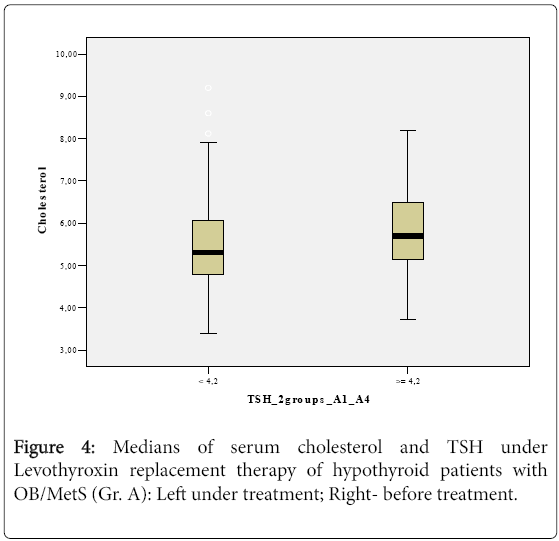
Figure 4: Medians of serum cholesterol and TSH under Levothyroxin replacement therapy of hypothyroid patients with OB/MetS (Gr. A): Left under treatment; Right- before treatment.
Despite of absence of a significant difference between the mean values of T-Cholesterol between both studied groups (P>0,05), hypothyroid patients revealed a significant correlation between TSH and T-cholesterol (P=0,029). These data might be explained by two factors. On the one hand most of the patients in gr. A had subclinical hypothyroidism. On the second hand dyslipidemia characterized obesity and metabolic syndrome most likely attenuate the difference between hypo and euthyroid patients.
Thyroid hormones have multiple effects on the regulation of lipid digestion, absorbtion, synthesis and catabolism. Much evidence shows that co-existence of hypothyroidism and obesity can result in severe hyperlipidemia leading to incresed risk of cardiovascular disease [13]. Serum lipids, glucose and thyroid hormones seem to interact according to a more complex mathematical function than previously expected [11,13]. Recently, several studies had reported that even relativly low thyroid function which was still within the normal range might be more dangerous in people with type 2 –DM [8,14,15].
Our data demonstrated that hypothyroidism significantly aggravated the lipid metabolism in patients with higher grade of Ob/ MetS. These disturbances co-existing with the high prevalence of arterial hypertension, type 2 diabetes and high BMI increase the cardiovascular risk to a great extent. The replacement L-T4 treatment applied in hypothyroid patients of Gr. A revealed a significant hypolipemic effects which might prevent the progression of subclinical to overt hypothyroidism and atherosclerosis.
The patients included in the study demonstrated that hypothyroidism and MetS/cOb are characterized by a variety of similar disturbances of metabolic regulation as insulin resistance (HOMA-IR) and chronic inflammation of adipose tissue resulting in increased CRP and adipocytokines overproduction as leptin. The association between circulating TSH levels and cardiovascular risk factors seems to be amplified by the degree of insulin resistance and leptin level [16].
Our data revealed the significant correlations between TSH, CRP, leptin and BMI which appeared concordant to systemic chronic inflammation and insulin resistance. In this respect thyroid hormone deficiency seems to be per se a possible pathogenetic factor aggravating the metabolic disturbances via adipocytokines overproduction in adipose tissue. These corresponded to recent data which elucidate the role of adipocytokines, especially leptin in the feedback between fat tissue and thyroid hormones [10,11,17,18].
All overweight and obese subjects and those with metabolic syndrome should be routinely screened for the thyroid dysfunction, including subclinical hypothyroidism, and treated accordingly to decrease cardiovascular risk. Most systemic population-based studies are needed in order to elucidate the pathogenetic interactions and etiological factors behind these processes.”