Research Article - (2015) Volume 3, Issue 2
Background: The use of medicinal plants as an alternative healthcare is widespread in developing countries. This is due to several factors ranging from the belief of the absence of side effects to the difficulty of access to allopathic medicines. Seen it, it is of utmost importance the study of the use of these medicinal plants and its relationship with allopathic medicine and the public health system. The objective of this study was to identify the range of natural health products and conventional drug therapies used by patients assisted by basic care units of the Brazilian Unified Health System.
Methods: Five basic health units in the city of Pelotas were select by a convenience sample and patients were interviewed about how were treated, including their use of natural products. The questionnaires have closed and semiclosed questions. The questionnaires have questions about the use of medicinal plants and if theirs use was concomitant with allopathic medicines.
Results: Most sample-comprising patients at basic health units (94.6%) reported using herbal medicine as an alternative and complementary therapy, and 64% also admitted growing some type of plant with medicinal purposes in their homes for their own use. Furthermore, 55.2% of patients taking herbal medicine to treat their illnesses did without the concurrent use of synthetic chemical drugs. 43.84% of interviewed patients were using some allopathic medicine daily. The possibility of interactions between anticoagulants and ‘boldo’ was found in the literature as well as the ‘lemon’ with chloroquine and also between ‘chamomile’ and anticoagulants and analgesics.
Conclusion: It is important to educate the public about the adverse effects of concomitant use of herbal and allopathic as these problems occur in the absence of knowledge of users, who often self-medicate with herbs, and health professionals who do not have sufficient clarity on the correct concepts of herbal medicine.
Keywords: Phytotherapeutic drugs; Complementary medicine; Public health; Herb-drug interaction; Adverse effects.
Herbal Medicine is a highly popular complementary or alternative mode of treatment with an annual turnover of US$ 60 billion with a constantly growing market [1]. As one of the top 10 consumers of herbal medicines, Brazil is believed to have about 66% of its population using medicinal plants as the only alternative for the treatment of their diseases. Some factors that contribute towards the spread of this therapy are the natural origin of the drugs, the belief in their safe use and the alleged lack of side effects [2].
The World Health Organization (WHO) has noted that it is important to incorporate modern with traditional medicine to implement health systems and improve the population´s health. Due to formally stimulated interest in medicinal herbs and traditional medicines, WHO has deemed it worthwhile to provide assistance to countries in their promotion of health programs which are better adapted to local socio-economic situations [3,4]. Several Brazilian states have already introduced the use of herbal medicines within the public health system [5-8]. According to the 2010 Brazilian Unified Health System´s official data, herbal therapy made its way into the government health system of sixteen Brazilian states [9].
Authors suggest that one of the major factors contributing to the increasing popularity of herbs in developed countries and the sustained use in developing countries is the perception that herbal remedies are efficacious, and in some cases more so than physicianprescribed allopathic medicines. This favorable level of perceived efficacy would support continued use, and in a significant number of patients, concomitant use with conventional allopathic medicines. This scenario, of concomitant herb-drug use, raises the growing public health concern of potentially harmful interactions [10].
It is known still that the indiscriminate use of medicinal plants and herbs is due to the lack of knowledge on their adverse effects. Almost one third of current users of herbal medicines do not know about the risk of herb-drug interactions [11]. A drug-herb interaction can be defined as pharmacologic or clinical response to the co-administration of a traditional drug or pharmaceutical preparation and a herbal product [12].The idea that herbal medicines have no adverse effects is erroneous and ignores the obvious fact that certain herbs may change the distribution and effect of certain allopathic medicines, affect their metabolism and eliminate the good effects of the formulations [1,2,13]. Moreover, it is clear that there is an increased risk of adverse interactions between herbal and allopathic medicines than between herbal medicines and synthetic drugs, which is due to the diversity of pharmacologically active chemical constituents in the medicinal herbs. On the other hand, synthetic drugs have unique chemical identities [14].
Further aggravating the problems reported above studies report that most herbal users did concomitantly with allopathic medicines, without the knowledge of your doctor [10,15]. The prevalence of drugherb interactions is extensive but unknown, signifying the negligence of the consumers in reporting adverse herb reaction or drug-herb interactions [16]. This practice can further consolidate the perception that this potentially dangerous practice is safe and encourage further concomitant use herb - drug uninformed ways [10]. There is an obvious importance of public awareness of the potential dangers of herb-drug combinations, as several studies show a relatively high incidence of adverse effects associated with this practice [10,17-19].
Due to the above issue, current investigation analyzes the main medicinal plants consumed by patients of the Brazilian Unified Health System in some basic health units of Pelotas RS Brazil, and verifies possible interactions between medicinal herbs and allopathic medicines.
The municipality of Pelotas in the southern state of Rio Grande do Sul, Brazil, on the banks of the São Gonçalo Canal, at 31°46'19 " S and 52º20'33'' W, has an area of 1,921.80 square kilometers, at an altitude of 7 mts, featuring a typical humid subtropical climate. Pelotas has a population of 323,034 inhabitants, including 22,082 residents in the countryside. The municipality´s economy consists of agribusiness and trade [20].
Half-structured and structured questionnaires were carried out during one year in five Basic Health Units (BHUs) in Pelotas, selected according to their importance, diversity of service and location in the municipality so that the covering of a more diverse population and an expansion of the investigation could be achieved. The questionnaire was performed by two students previously calibrated within the pilot project. A previous meeting was held to eliminate doubts with regard the questions of the questionnaire and possible responses. The questionnaire could be adjusted and uniformity between the interviewers could be obtained. Selection condition was that subjects were patients attended by the Brazilian Unified Health System. The project was approved by the Committee for Ethics in Research of the Faculty of Dentistry, Federal University of Pelotas (Resolution 083/2009). The patients were randomly chosen, asked whether they wanted to participate in the research and then interviewed while they were waiting for their respective health service. All interviews were conducted after the signing of the consent form.
The questionnaire aimed to report the socio-economical characteristics of the informants to link the use of medicinal plants with income, age and gender, for a comparison with other similar studies. It also investigated the botanical and ecological characteristics of plants used for medicinal purposes and their alleged therapies to identify possible drug interactions.
Information on each plant was registered, or rather, its name, section of the plant used, preparation and storage methods, season in which it was harvested, its alleged therapeutic purposes, information on herb administration (frequency, concomitant use with allopathic medicines, effects) and duration of the treatment.
Formal interviews and some occasional conversations with 333 people were performed. After the application of the questionnaires, data were tabulated and analyzed.
The use values (UVs) [21] for each plant were also collected. For this measurement, we used the formula UVIS=( Uis)/nis, where Uis is the number of uses mentioned by the interviewee for the species, and nis is the number of interviews with the informant. The UVIS and Uis values were the same in our experiment, as only one interview was conducted with each interviewee. To calculate the value of use of each of the species, the UVs were used in the formula UVs = UVIS/n, where UVIS equals the value to an informant of using a particular plant species, and is the total number of informants interviewed. Any interviewee could cite all species.
A descriptive statistical analysis was performed using the SPSS version 10.0 software package, and the Chi-square test was used. Significant differences were accepted at the p<0.05 value.
In this article, a literature overview is provided of known or suspected interactions of the plants considered important by the population studied with conventional allopathic therapies.
Most sample-comprising patients at basic health units (94.6%) reported using herbal medicine as an alternative and complementary therapy, and 64% also admitted growing some type of plant with medicinal purposes in their homes for their own use. Further, 55.2% of patients taking herbal medicine to treat their illnesses did so without the concurrent use of synthetic chemical drugs. In fact, 43.84% of interviewed patients were using some allopathic medicine daily, with a prevalence (46.6%) of hypertension drugs. A mere 3.42% of the sample revealed that they make use of allopathic medicines without the use of herbal medicine as a complementary treatment (Table 1).
| Herbal Medicine | |||
|---|---|---|---|
| Allopathic Medicine | Use | No use | Total |
| Use | 141 96.58% | 5 3.42% | 146 100% |
| No use | 174 93.05% | 13 6.95% | 187 100% |
| Total | 315 94.59% | 18 5.41% | 333 100% |
Table 1: Absolute and relative frequencies of use of herbal medicine associatedwith allopathic drugs.
Since the sample was predominantly (84%) female, “gender” had a significant role in the choice of herbal medicine as a form of therapy (p=0.008). However, the option for the use of allopathic drugs was not correlated with the respondents´ gender (p=1).
Most interviewed patients were within the 41-50 year old (21.02%) age bracket, followed by the 21-30 year old (20.42%) age bracket. A breakdown in percentages for herbal use occurred at different ages (p=3.6) in the case of treatment of signs and symptoms of the disease, or rather, there was a significant correlation between age and use of herbal medicines. The same factor was also observed for cases in which allopathic drugs were used (p=2.8).
Most interviewed patients (64.3%) had an income between US$ 269-537 although family income did not seem to be decisive in the decision to use herbal and allopathic medicines (p=2.3).
Moreover, the patients interviewed were free to talk about which plants they used for the treatment of various diseases (Figures 1 and 2). Direct objective questions were used and the following results were obtained: 52.9% reported using herbs for pain relief; in fact, 27.1% cited the use of macela (Achyrocline satureoides Lam) for this purpose. Twelve percent reported the use of teas to treat diabetes, with 43.9% using the “insulin” (or princess) vine (Cissus sicyoides L) for this purpose. On the other hand, 34% reported the use of teas to treat toothache: the common Malva (Malva sylvestris L.) was the plant used by 86.7% of interviewed patients. About 50% of patients used some herbal remedies to treat sore throat, with 51.6% using the ‘Tansagem’ (Plantago spp, Plantago major) for this purpose. The groundsell (Baccharis genistelloides) against obesity and overweight was cited by 25.3% of interviewed patients, whilst 22.5% reported the use of teas for the same purpose. About 20% of users treated thrush or herpes with the flower of the black elder (Sambucus nigra L.) (95%). Forty percent used plants to treat any type of inflammation and the common mallow (Malva sylvestris L.) was used by 46% of interviewed patients. Only 21.3% used herbal medicines to treat injuries and a type of aloe (Aloe arborescens Mill) was the most used (36.6%).
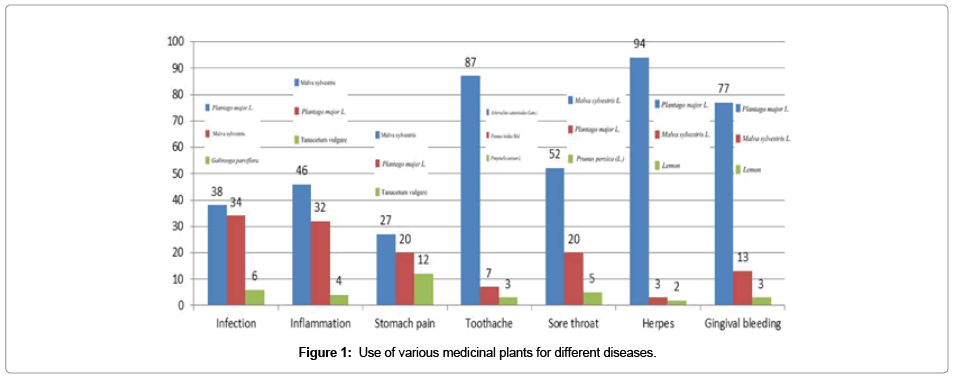
Figure 1: Use of various medicinal plants for different diseases.
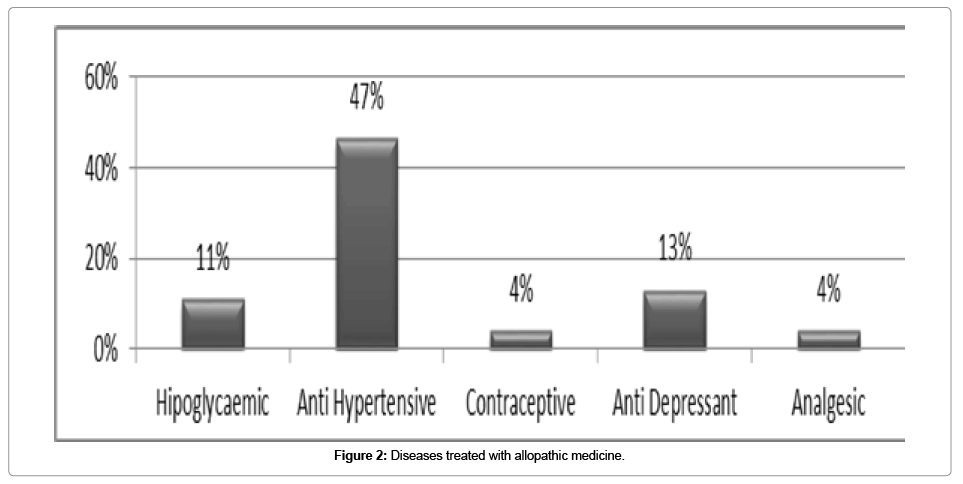
Figure 2: Diseases treated with allopathic medicine.
In current study 65 different plants were reported against different types of illnesses, of which the common mallow (Malva sylvestris L.) was the most cited (29.6%) specifically for dental pain (31.1%). Infection (55.3%) was the most frequent symptom reported which occasioned the use of herbal plants and plantain (Plantago spp, Plantago major) was the most cited plant to treat this problem (37.3%).
In current study, the importance of each medicinal plant for the community under analysis was obtained by calculation, or rather, the higher the number of usages of the medicinal herb, the more important it is for the community. This fact was considered relevant for the review of the literature review on possible drug interactions, adverse reactions and contraindications. The ten plants considered important by the population studied are given below in the use value order:
1. Common mallow (Malva sylvestris L.)
2. Plaintain (Plantago spp.)
3. Macela (Achyrocline satureioides)
4. Boldo (Peumus boldus)
5. Black elder (Sambucus nigra L.)
6. Groundsell bush (Baccharis genistelloides)
7. Lemon balm (Melissa officinalis)
8. Tansy (Tanacetum vulgare L.)
9. Aniseed (Pimpinella anisum)
10. Camomile or chamomile (Matricaria recutita L.)
The ten above-mentioned plants were analyzed for their possible drug interactions or adverse effects found in the literature.
Most respondents (94.6%) reported knowing and using medicinal plants for the treatment of various signs and symptoms of different diseases for themselves and their family. These data are consistent with other studies that demonstrate the widespread use of plants for medicinal purposes. Brasileiro et al [22] studied the population assisted by the Family Health Strategy in Governador Valadares MG Brazil, and found that 91.9% of the interviewed frequently used herbs to treat diseases, whereas only 8.1% did not. The indiscriminate use of medicinal plants is due to the fact that users are not aware of the adverse effects they may produce. Mahady et al. [23] reported that 65% of individuals claimed that herbal medicines were a safe therapy. The safety concept is highly misleading in the case of most plants used as medicinal since many have significant toxic side effects [24]. To make matters worse, they also registered that 70% of patients who used herbal medicine as treatment did not report the fact to their physicians or health professionals [15]. Consequently, no monitoring of drug interactions occurs since the concomitant use of two drugs is not acknowledged [25].
Current study showed that users reported that they have some medicinal plants at home (64%). The use of medicinal plants is facilitated when the patients grow the plants and probably use them fresh [22]. Another interesting information is that 55.2% of respondents exclusively use medicinal plants to treat their illnesses. It is a well-known fact that Brazil is one among the ten countries that most consume plants for medicinal purposes [26]. In addition to such a high demand, few studies characterize the exclusive use of medicinal plants by Brazilians. These individuals primarily endeavor to heal their illnesses and those of their families at home, without any medical supervision. If the symptoms do not disappear, they seek medical advice and take the prescribed synthetic drugs. This behavior is either due to drug prices or to the unavailability of the free medicine by the health care system [27].
Many patients interviewed (43.8%) claimed using allopathic medicines regularly. The costs of drugs have a similar pattern with spending on health care, or rather, the poorest people, with more morbidities and therefore requiring a greater need of drugs, tend to spend less. The restriction in the use of drugs among people with low purchasing power becomes evident when one notes that the weight of spending on household income is proportionally greater than that for people with higher incomes [28].
The most common pathology was arterial hypertension (46.6%) and agrees with the same trend found by Lima-Costa et al. [29] in a PNAD description among patients of the Brazilian National Health Care system. Only 3.42% of the sample made use of allopathic medicines without herbal medicine as complementary treatment. This result is very similar to research by Peng et al. [30] where about 43% of herbal medicines users also took synthetic drugs concomitantly; 52.2% only used herbal medicine against disorders; 1.5% used only allopathy; and 4% did not use any of the two forms of treatment. Unfortunately, there is a great lack of studies on the use of allopathic and herbal medicines in Brazil so that a greater importance to the issue could be provided.
Most of the interviewed in the sample were females (84%). The gender characteristic was highly significant in the use of herbal medicine as a form of therapy (p=0.008), since the option for the use of allopathic drugs was not correlated with the gender of the respondents (p=1). The predominance of females has already been reported in the literature. In fact, as a rule, women are responsible for the cultivation and preparation of medicinal plants. They are also responsible for the feeding and care of children or other family members when they become ill [8].
The age group of most respondents lay in the 41-50 years age bracket (21.02%), followed by the 21-30 years age one (20.42%). Again there was a breakdown of herbal use, at different ages, for the treatment of signs and symptoms of diseases with no significant correlation between a certain age and use of herbal medicines. Since there was no exclusion or inclusion of respondents by age, the respondents´ age groups were very comprehensive (20 years above 60 years old). Other studies have reported that people over 30 years were more open to discuss the use of medicinal plants, while young people would prefer to use chemically synthesized drugs and showed various levels of disbelief in the healing power of medicinal plants [27]. Several authors have shown that the knowledge and use of medicinal plants is not only undergoing a gradual decline but any knowledge of medicinal plants is restricted to communities in rural areas [31-33]. Current data differed with regard to results of the less than 20-year-olds who featured 91% of supporters of herbal medicine. Percentage rose to 96% among people within the 20 - 30-year-old brackets.
Respondents (64.3%) had predominantly an income between 1 and 2 Brazilian minimum wages or US$ 269-537. Some studies have linked the use of herbal medicines with high schooling levels and income in developing countries such as Brazil [34]. However, current study was restricted to users of the government health system who have lower income levels and schooling [34].
Respondents were free to mention the plants used for the treatment of diseases. Most reported using the plaintain (Plantago major) in the treatment of infections, with a 38% preference, followed by the common mallow (Malva sylvestris L.) (34%) and by the potato weed (sometimes called gallant soldier) (Galinsoga parviflora Cav.) (6%). The common mallow (Malva sylvestris L.) was the favorite plant against inflammation (46%), gingival bleeding (77%) and toothache (87%). The macela (Achyrocline satureioides) was the most cited plant for the treatment of stomach pain (27%), followed by boldo (Peumus boldus) (20%) and aniseed (Pimpinella anisum) (12%). In the case of sore throat, the tansy (Tanacetum vulgare L.) was mentioned by 52%; the common mallow (Malva sylvestris L.) by 20% and lemon by 5%, in the users´ preference. For the treatment of herpes the most mentioned plant was the black elder (Sambucus nigra L) with 94%, followed by aniseed (Pimpinella anisum L.) with 2%.
The common mallow (Malva sylvestris) was one of the most cited plants in the study. In the literature, the mallow is mentioned as a drug against inflammation, fever, diseases of the bladder and throat and for general infections, ovarian infections, cystitis, genital cleansing, mouth wounds and wounds in general. It is also employed as a bronchodilater, expectorant, anti-tussive and anti-diarrheal medicine. The mallow is also highly recommended for acne and skincare and as an antiseptic, emollient and demulcent [35]. Due to these properties, the use of this plant in the prophylaxis and periodontal treatment of oral and pharyngeal irritation is widespread [36]. No type of harmful interaction with the common mallow has been found or documented in the literature. In fact, the National Health Surveillance Agency, through its Resolution RDC 17 issued on February 24, 2000, confirms the effectiveness of Malva sylvestris, unaware of its toxicity [37].
'Tançagem' (Plantago major) was the most frequently cited medicinal herb by the interviewed in current study for the treatment of infections. There are reports in the literature on the use of this plant for the treatment of nasopharyngeal inflammation [38]. Other studies also report that 'tançagem' (Plantago major) is used in the treatment of several diseases such as skin diseases, infectious diseases, digestive, respiratory, reproduction, blood circulation problems, and the relief of pain and the reduction of fever against tumors [39]. Scanty information exists in the scientific literature on the plant´s adverse effects and drug interactions. Several Internet sites report on its adverse effects and mention arrhythmia, heart arrest, allergic reactions and irritations.
The macela (Achyrocline satureioides) is the most commonly used drug against stomach pain and is commonly used in folk medicine as a tea to treat digestive problems and inflammation. Infusions of A. satureioides flowers are widely used in Brazilian folk medicine as a digestive, antispasmodic, anti-inflammatory and hypoglycemic agent for the treatment of gastrointestinal disorders and for the decrease of blood cholesterol levels. Although some previous studies are extant, the toxic effects of A. satureioides extracts are little known. In a study using hematological Achyrocline satureioides (Lam.) DC in mice, Martins et al. [40] detected macrocytosis, eosinopenia, neutropenia and lymphocytosis.
The boldo (Peumus sp) was the second most commonly cited herbal medicine to treat stomach pain, due to alkali boldine confirmed by many reports [41]. Boldine and boldo extracts are known for their hepatoprotective and choleretic properties which stimulate the bile flow [42]. In addition to its beneficial activities on the gastrointestinal tract, boldine exerts anti-inflammatory and antipyretic responses. The boldine is an effective inhibitor of prostaglandin synthesis [43] responsible for pain transmission. The interaction between warfarin and boldo may be found in the literature. Warfarin is an antivitamin K (AVK) drug or oral anticoagulant and may interact with different anticoagulant actions of herbal medicines such as the boldo. In one case reported in the literature the boldo-warfarin interaction just increased the anticoagulant parameter in a 67 year old patient [44].
The black elder (Sambucus nigra), a plant cited by respondents in current research for the treatment of herpes simplex virus (HSV- 1) commonly associated with facial sore outbreaks, seems to be effective against the virus. In a study by Morag [45] an extract from Sambucus nigra was tested against HSV-1 and demonstrated to have completely inhibited the replication virus strains. The black elder may strongly stimulate the immune system by inducing cytokine production in healthy subjects and in patients with influenza, or in other immunocompromised patients, such as those with cancer or HIV. Formulas containing Sambucus have a strong stimulating effect on the production of anti-inflammatory and inflammatory cytokines (IL-1β, TNFa, IL-6, IL-8, IL-10). The production of all 5 cytokines by a drug containing Sambucus increased between 1.3 and 1.6 times when compared to the placebo [46]. No type of interaction with the Sambucus nigra was found in the literature about which it is well documented.
The groundsell bush (Baccharis genistelloides) is commonly used to treat liver problems, digestive disorders, malaria, ulcers, diabetes, anemia, diarrhea, urinary inflammations, tonsillitis, worms, hypercholesterolemia, erectile dysfunction, female infertility and rheumatism. It is also used as an abortive drug [47]. The main use of the groundsell in current study was the disappearance of digestive disorder symptoms. The main toxic effects reported for B. genistelloides is the induction of abortion, commonly reported and experimentally proven in animals, attributed to an uterotonic activity of its compounds [48]. Although studies fail to indicate any problems with kidney or liver toxicity, the use of the groundsell should be prohibited for pregnant women due to its proven abortion risks and for patients on drugs for blood pressure due to its hypotension effects [49].
The lemon balm (Melissa officinalis) was mentioned by the interviewed for the treatment of intestinal and menstrual cramps. The literature reports that that lemon balm may interact with other medicines containing herbs, especially kava (Pipermethysticum G. Forst). In fact, it interacts with depressants on the central nervous system and on thyroid hormones (thyrotropinreleasing hormone) [50].
There are few studies on the adverse reactions and contraindications for the tansy (Tanacetum vulgare L). Empirical information was more abundant than scientific information and it is believed that one should be careful with the plant´s consumption by pregnant women, infants and children. The components of the tansy, such as tanecetona acid, are toxic. High doses may cause poisoning and the necessary cautions in its consumption are highly recommended.
The aniseed (Pimpinella sp), the third plant used for stomach pain, is used to treat heartburn, stomach ache, digestion difficulties and dyspepsia [50]. No interactions with the aniseed were found in the literature which is well documented on the subject.
The chamomile (Matricaria recutita) is mostly used as a tranquilizer. In a study by Farnsworth (1972) [51], in which flavored oil of chamomile was used, it was shown that it had a sedative effect and a positive effect on mood. The flavonoid apigenin, found in chamomile, proved to be a ligand for central benzodiazepine receptors exerting anxiolytic and slight sedative, albeit not anticonvulsant or myorelaxing [51,52]. The interaction between chamomile anticoagulants and cyclosporine is found in the literature. Seagal and Pilote [52] report that one patient who intook warfarin had severe internal injuries after using chamomile, probably due to coumarin compounds which act synergistically with warfarin, resulting in supratherapeutic anticoagulation. In another study, one patient had a high concentration of cyclosporine after drinking from 1 to 1.5 L/day of tea. When the same patient ceased ingesting the tea, concentrations returned to their former level [53]. The use of aspirin as a painkiller should also be taken into account by patients. Since ASA has anticoagulant-antiplatelet properties, the same type of interaction that occurs with warfarin as an anticoagulant may also occur with this drug. In addition, allergic reactions to this plant are not uncommon. These reactions include symptoms such as abdominal cramps, tightness in the throat, angioedema of the lips and eyes, hives, itching, upper airway obstruction and pharynx edema [54].
Several other plants were cited in current study besides those mentioned above, or rather, within the list of the ten major plants reported by the population. Due to the importance of the topic and to the lack of extant studies on the subject, a review of the literature on other medicinal plants cited in current study but not part of the ten most important ones will follow.
• The aloe (Aloe arborescens) was mentioned by the interviewed patients primarily as a treatment for gastritis symptoms by drug infusion. Documented in the literature, there is no drug interaction when the medicinal plant is used, although some adverse effects such as contact dermatitis are mentioned [55]. In addition, it is contraindicated for pregnant women, breastfeeding mothers and children [55,56], intestinal obstruction, ulcerative colitis, appendicitis, abdominal pain of unknown origin [57], hemorrhoids and kidney diseases [58] .
The leaves of the sweet orange (Citrus sinensis L) were used as an infusion for the treatment of pain and bronchitis. The literature mentions allergies (caused by volatile oils of fruits and flowers) [59], erythema, blisters, pustules, skin and pigmented spots (caused by furanocumarins found in the juice and peels of fruits) [60] as adverse reactions. Its use is contraindicated during pregnancy and lactation [61].
• Fennel leaves (Foeniculum vulgare Mill.) were prepared by infusion and used for the treatment of insomnia. Some therapeutic uses of the plant have been proven. They include coughs, bronchitis [56,57,62], mild gastrointestinal problems with spasms in the upper respiratory phlegm and flatulence [56]. One study suspects a likely interaction between ciprofloxacin and Foeniculum vulgare, with reduces plasma concentrations of the antibiotic [62].
• The leaves of the Brazilian cherry (Eugenia uniflora) were used by the interviewed patients to treat bleeding gums. The literature shows a contraindication in its use for patients with arrhythmias and heart failure [61].
• The lemon, often in the form of juice, may also be used for the treatment of throat pain due to its antimicrobial action, probably because it contains citral and linalool [63,64]. A drug interaction was detected between the lemon and chloroquine, a drug used for the treatment and the clinic prophylaxis of malaria [65]. In the interaction, plasma concentration of chloroquine is reduced and its therapeutic effects decreased [65]. Another interaction occurred with Fe which may increase iron absorption by the body [66].
Further studies addressing this issue are necessary, coupled to a conscience-raising education policy for the population, both to users of herbal medicines and to health care professionals, with regard to the high potentiality in the adoption of this practice.
It is important to educate the people on the adverse effects of the concomitant use of herbal and allopathic medicines as these problems occur without the users´ awareness. This is more serious because people tend to self-medicate themselves with herbal medicines and health professionals do not have sufficient knowledge on their correct use.
SGDO was responsible for the administration of the questionnaires; she analyzes the results, literature, writing, and review of the scientific paper. RGL and EP were responsible for the administration of the questionnaires; they analyze the results, literature, writing and review of the scientific paper.
